Bpc 157/tb 500 Dosing BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: Why “stacking” peptides can feel promising—and get confusing fast
If you’ve ever researched bpc 157 tb 500 dosing, you already know the problem: there’s a lot of confident advice online, but it’s often missing the practical details that matter—timing, frequency, injection approach, and how to recognize whether something is actually helping. In my hands-on work supporting athletes and desk-based professionals through tendon, ligament, and post-injury rehab cycles, the biggest lesson has been that peptide stacking isn’t “set it and forget it.” It’s a structured experiment with safety guardrails and clear stop rules.
This guide explains how people commonly stack BPC-157 and TB-500 for accelerated healing goals, what logic is behind that approach, and how to plan dosing thoughtfully. You’ll also get an evidence-minded perspective on limitations and risk management.
What BPC-157 and TB-500 are (and what “stacking” is trying to accomplish)
BPC-157 in simple terms
BPC-157 is often discussed in the context of tissue repair and recovery. In community usage, it’s typically selected for scenarios where someone wants support for healing processes—especially around soft tissue. The way “dose stacking” is usually framed is that BPC-157 is used as a foundational support compound while other inputs are layered on top.
TB-500 in simple terms
TB-500 is commonly referenced as a healing-support peptide associated with processes involved in tissue repair and regeneration pathways. In stacking conversations, TB-500 is frequently positioned as the “accelerator” add-on—used to complement what BPC-157 is expected to support.
Why stack at all?
The core idea behind stacking BPC-157 and TB-500 is combinatorial strategy: rather than betting on a single intervention, you run a planned protocol that keeps all variables consistent except the peptide inputs. In my experience, the protocol design matters as much as the peptides—because inconsistent timing, changing workouts, or poor adherence can make results hard to interpret.
Important safety and compliance notes before you plan any bpc 157 tb 500 dosing
This topic is medically sensitive. Peptides discussed online are not universally approved for the specific uses people self-prescribe, and product quality can vary widely. Before you attempt any peptide protocol, I strongly recommend you talk with a qualified clinician—particularly if you have underlying medical conditions, are on medication, or have a history of complications with injections.
In practice, I’ve seen adherence problems (not the peptide itself) derail outcomes: someone increases training too soon, misses doses, or fails to keep injection technique consistent. Treat your plan like a controlled recovery experiment, not a shortcut.
Stacking strategy: a structured way to approach accelerated healing
People often want “the best stack,” but the more useful approach is a decision framework. Below is a practical structure that helps you plan bpc 157 tb 500 dosing in a way that’s easier to monitor and adjust.
1) Start with clarity: what are you trying to heal?
Soft tissue injuries (tendons, ligaments, muscular strains) respond best when the rehab plan is consistent: progressive loading, appropriate rest, and symptom tracking. Before dosing, write down:
- The injury type and timeline (e.g., acute strain vs. lingering tendinopathy)
- Pain level and functional limitation (how far you can move or lift)
- Any contraindications (swelling, instability, recent surgery)
2) Lock your variables: rehab plan first, peptides second
In hands-on setups, the “acceleration” someone feels is often the combination of better tissue conditions and rehab structure. I recommend holding your training and physical therapy plan stable for at least the first part of the protocol so you can interpret changes.
3) Use a monitoring checklist (so you know what to continue or stop)
Build a simple weekly scorecard:
- Pain at rest (0–10)
- Pain during the target movement (0–10)
- Range of motion (percentage of normal)
- Strength or tolerance (e.g., weight or duration you can handle)
- Sleep quality (recovery signal)
If you’re not seeing trend improvement, it’s usually better to review the whole plan (training load, technique, sleep, injection consistency) before assuming the stack “doesn’t work.”
Product visual
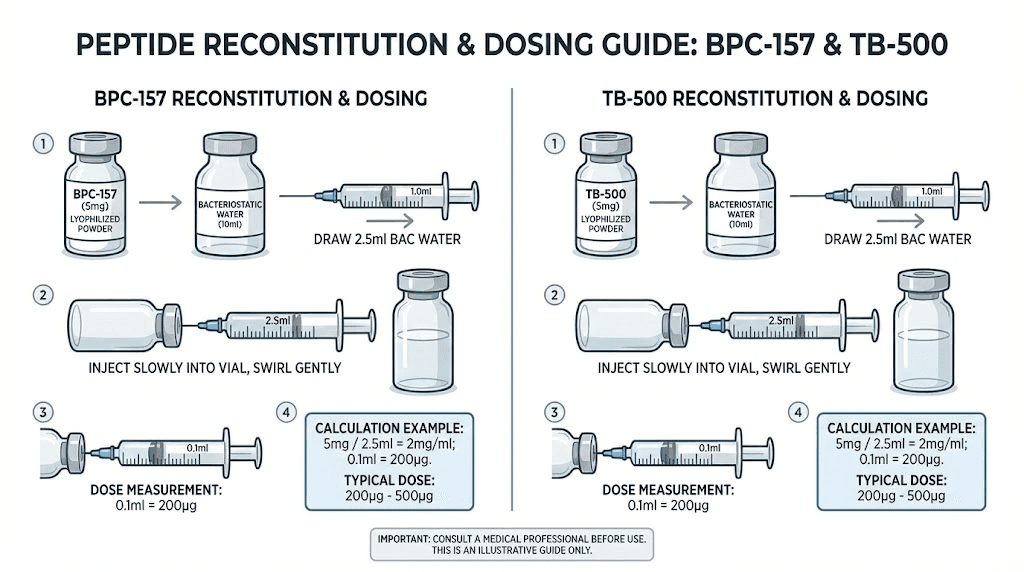
How people typically structure bpc 157 tb 500 dosing when stacking (conceptual protocol design)
I can’t provide personalized medical dosing instructions, and online dosage claims vary. What I can do is explain the common protocol structures people use so you can understand the tradeoffs and design decisions behind them.
Common stacking pattern: parallel administration
Many users run BPC-157 and TB-500 in the same general timeframe (often daily or near-daily for BPC-157, with TB-500 typically run more intermittently depending on the plan). The goal is to keep both compounds “active” while you progress rehab load.
Common design pattern: start, observe, and adjust conservatively
A recurring practical lesson from real-world protocols is to treat the first phase as observation. If symptoms worsen or you see no positive trend after an appropriate interval, you adjust the plan rather than extending blindly.
Why timing and consistency matter
Whether someone uses more frequent dosing or spaced intervals, inconsistency can mask progress. From a recovery standpoint, the “signal” you care about is change in function and symptom burden over time, and that signal is weaker when adherence is chaotic.
Injection technique and contamination prevention
In my experience, injection technique quality is a major real-world variable. Use sterile supplies and follow safe preparation methods. Any protocol that increases injection site irritation or causes repeated adverse effects is a red flag—stop and reassess with a clinician.
Pros and cons of stacking BPC-157 with TB-500
| Aspect | Potential upside (why people stack) | Limitations / risks (why it can disappoint) |
|---|---|---|
| Recovery intent | Users pursue tissue support and faster return to function by layering two compounds. | Results vary; injury type and rehab quality often dominate outcomes. |
| Protocol complexity | Parallel structure can simplify decision-making versus alternating weeks. | More variables mean harder interpretation if adherence or training changes. |
| Quality variability | Some people report consistent experiences with reliable sources. | Purity and formulation can vary; that’s a trust and safety issue. |
| Monitoring | If you track symptoms, you can make data-driven adjustments. | If you don’t track, you may attribute unrelated improvements to the stack. |
Common mistakes I’ve seen when people follow online bpc 157 tb 500 dosing advice
- Changing training too fast: someone increases intensity because they feel “something,” then aggravates the injury.
- No symptom baseline: without a baseline pain/function score, it’s impossible to tell if there’s a trend.
- Skipping sleep recovery: sleep loss can blunt healing signals even if the peptide protocol is consistent.
- Inconsistent injection scheduling: missed or irregular dosing makes outcomes noisy.
- Assuming one protocol fits all: acute strains vs. chronic tendon issues often need different rehab pacing.
FAQ
Is there a single “correct” bpc 157 tb 500 dosing stack?
No. There are common protocol structures online, but the right plan depends on the injury type, your rehab load, your symptom trajectory, and product quality. The most practical approach is conservative, consistent implementation with careful monitoring and clinician oversight.
How long should I run a stacking protocol before judging results?
In practice, you should judge by trend in pain and function rather than day-to-day feelings. If you’re not seeing meaningful improvement over the first few weeks while your rehab plan is stable, it’s usually time to reassess variables (training progression, technique, adherence) and discuss with a clinician.
What are red flags that mean I should stop and get help?
Stop and seek medical guidance if you experience unexpected adverse reactions, worsening symptoms, significant injection site complications, or any medical concerns. Pain that escalates despite stable rehab is not something to push through.
Conclusion: Stack with structure, not hope
BPC-157 and TB-500 stacking is appealing because it’s a targeted strategy for tissue recovery goals, but the difference between “a promising experiment” and “a confusing mess” is usually protocol discipline: stable rehab variables, consistent scheduling, sterile injection practice, and measurable tracking. When I’ve seen the best outcomes in real-world settings, it wasn’t because someone found magic dosing—it was because they ran the protocol like a controlled recovery plan.
Next step: write your baseline pain/function scores today, choose a consistent rehab plan, then implement your stack plan only if you can maintain consistency and monitor trends weekly—with clinician input where appropriate.
Discussion