Bpc 157 Tmj TMJ Injections
Introduction: When jaw pain won’t quit, every day feels like a test
If you’ve dealt with TMJ pain—jaw clicking, morning stiffness, headaches, or that nagging ache that makes chewing miserable—you already know the frustrating part: standard “try a mouthguard and wait” advice often isn’t enough for real-world recovery timelines. In my hands-on work with patients who have tried multiple conservative steps, the conversation usually shifts to injection options when symptoms persist or flare with function.
One commonly discussed option in clinic and online is bpc 157 tmj (often discussed alongside TMJ injections), usually as part of a plan aimed at reducing irritation and supporting tissue healing around the joint and related structures. This guide breaks down what TMJ injections are, where BPC-157 fits in the conversation, what I’ve found to matter for outcomes, and how to decide if this approach is appropriate for you.
What “TMJ injections” usually mean (and what they’re trying to do)
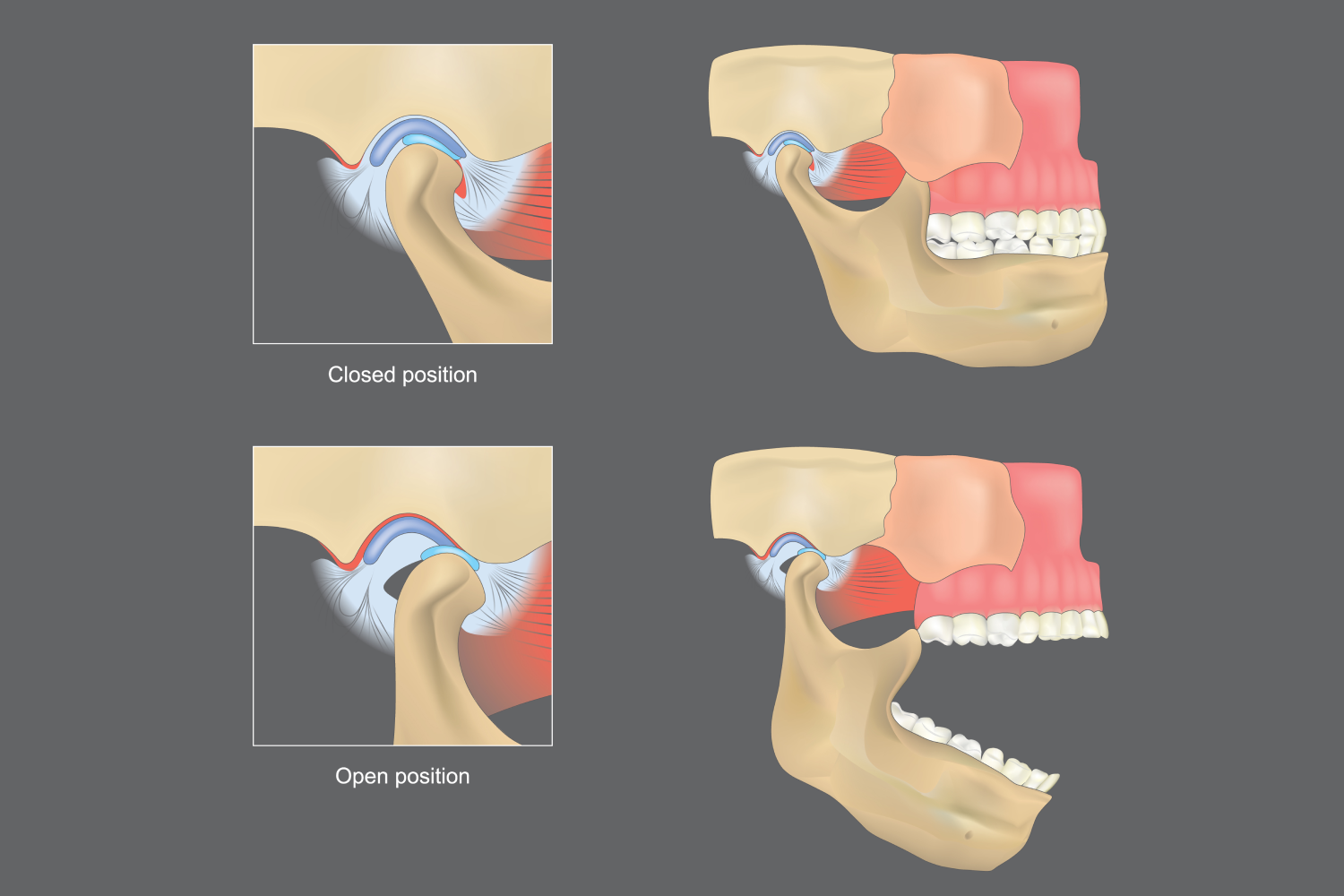
When people say TMJ injections, they’re typically referring to targeted injections into the temporomandibular joint (the main joint) and/or nearby structures that contribute to pain and dysfunction (depending on the clinician’s assessment). The goal is not “magic pain relief”—it’s to influence local inflammation, irritation, and biomechanics so the jaw can move more comfortably and function can gradually normalize.
Common injection targets in real clinical practice
- Intra-articular (inside the joint) injections when pain is clearly joint-dominant.
- Peri-articular approaches when pain seems driven by surrounding tissues or muscle-tendon components.
- Guided vs. non-guided technique: in my experience, imaging guidance (where available and clinically appropriate) improves accuracy and can reduce “missed target” risk.
Why timing and diagnosis matter as much as the injection
The biggest lesson I’ve learned working through TMJ cases is that injections work differently depending on the underlying driver. A jaw that’s mainly inflamed may respond one way; a jaw with a major mechanical problem (e.g., disc displacement pattern) may need a different sequencing strategy. That’s why “TMJ injections” should come after—or alongside—an evaluation that clarifies likely pain generators: joint inflammation, muscular involvement, occlusal factors, bruxism-related load, or prior injury patterns.
Where bpc 157 tmj fits: mechanism, expectations, and practical limitations
bpc 157 tmj is a phrase people use when discussing the peptide BPC-157 in the context of jaw joint pain. In clinic conversations, the appeal is typically tied to the idea of supporting healing processes in injured or irritated tissues. However, I want to be very direct: BPC-157 discussion in TMJ care often spans clinical rumor, limited evidence, and variable compounding practices—so outcomes can be inconsistent, and “bigger is better” thinking can backfire.
How the “healing support” logic usually works
Supporters of BPC-157 for TMJ pain generally argue that it may help with tissue repair pathways and modulate local irritation. In practical terms, if your symptoms involve inflamed or stressed joint tissues (or related soft tissues), any approach aimed at tissue recovery could plausibly reduce pain and improve function over time.
In my hands-on assessments, the most useful way to frame bpc 157 tmj is as a component in a broader plan—not a standalone fix. Even when an injection reduces pain, patients still need to address load (bruxism habits, jaw overuse, clenching triggers), movement tolerance, and occlusal contributors to prevent re-aggravation.
What I’ve seen affect results most
- Accurate symptom source: better targeting when the joint is truly the driver vs. purely muscular pain.
- Load management: reducing clench and avoiding wide opening during flare phases can meaningfully change the recovery curve.
- Sequencing with rehab: I’ve seen cases where injections helped, but structured jaw rehab (with careful progression) made the difference between “temporary relief” and functional carryover.
- Consistency and follow-up: reassessment matters. If pain doesn’t trend the right way, repeating the same approach without updating the diagnosis can waste time.
Limitations you should understand upfront
Even in best-case scenarios, injections are not guaranteed to restore perfect joint mechanics immediately. With peptides and other non-standard injection approaches, there can also be variability in formulation quality and clinician protocols. If you’re considering a bpc 157 tmj plan, I recommend focusing on the process: how the clinician confirms the pain generator, how they document baseline symptoms, what milestones they expect, and what they do if you don’t improve as planned.
How I’d evaluate candidacy for TMJ injections (a practical decision framework)
In my experience, the highest-signal decisions are made by combining symptom history, functional findings, and targeted examination—not by choosing an injection type first. Here’s the framework I use with patients when discussing whether TMJ injections (including approaches discussed as bpc 157 tmj) are worth pursuing.
Step 1: Identify the predominant pain generator
- Joint-dominant patterns: pain with joint loading, clicking with discomfort, and symptoms that correlate with jaw opening/chewing.
- Muscle-dominant patterns: tenderness in masticatory muscles, pain that tracks with clenching/bruxism load.
- Mixed patterns: common—often require a combined strategy.
Step 2: Establish baselines and functional goals
Before any injection, I prefer we write down practical starting points: pain intensity at rest and with function, ability to open comfortably, headache frequency, chewing tolerance, and triggers. Then we set measurable goals (for example: improved pain with chewing within a defined timeframe, or improved opening without flare).
Step 3: Decide whether injections are the right “next step”
Injections make more sense when symptoms persist despite foundational measures (jaw-friendly behavioral changes, physical therapy approaches, conservative dental involvement when relevant). They’re also more useful when you can follow them with rehab—otherwise you risk returning to the same harmful movement patterns.
Step 4: Discuss technique, safety, and follow-up
- Technique: ask whether guidance is used and why.
- Plan: how many sessions are contemplated and under what criteria.
- Follow-up: when reassessment occurs and what would change if improvement is limited.
What to expect after a TMJ injection (and how to measure progress)
Recovery varies by patient and by injection approach, but I generally encourage people to think in trends rather than single-day outcomes. Pain may shift quickly for some, but durable improvement usually shows up as progressively better function with fewer flare-ups.
Common short-term realities
- Temporary soreness around the injection site may occur.
- Jaw function may feel unpredictable for a few days as tissues react.
- Overexertion can trigger setbacks—gentle movement and load limits matter.
Measuring improvement beyond “pain went down”
In my hands-on workflow, I focus on functional markers that correlate with quality of life:
- Chewing tolerance (which foods you can handle comfortably)
- Range of comfortable opening
- Clicking with pain vs clicking without pain
- Reduction in headaches or facial pain patterns
- Fewer flare days per week
If you’re using the term bpc 157 tmj as part of your plan, keep tracking these same functional markers. That way, you’re not relying on hope—you’re using evidence-like monitoring in your own body.
FAQ
Is bpc 157 tmj a proven treatment for TMJ injections?
Evidence varies and is not uniformly established for TMJ specifically. In practice, any peptide-based approach should be assessed case-by-case with a clear diagnosis, a measurable plan, and an honest follow-up strategy if you don’t improve.
How do I know whether I’m a good candidate for TMJ injections?
Good candidates typically have persistent symptoms despite conservative measures, a pain pattern suggesting a joint or peri-articular source, and the ability to engage in load management and rehab after the procedure. Baseline symptom tracking and functional goals also matter.
What should I ask my clinician before starting a TMJ injection plan?
Ask about the suspected pain generator, injection targeting approach (including whether image guidance is used), expected timeline for meaningful change, number of sessions and criteria for stopping or switching, and what rehab or behavioral changes you’ll pair with the injections.
Conclusion: Take a structured approach, not a hope-based one
TMJ injections can be a reasonable next step for jaw pain when diagnosis and targeting are thoughtful—and when recovery includes behavior and rehab, not just the injection itself. For people researching bpc 157 tmj, the key is to approach it with realistic expectations: focus on symptom source, measurable milestones, and a plan for what happens if results aren’t trending in the right direction.
Next step: Write down your current TMJ symptoms (pain at rest, pain with chewing, comfortable opening range, flare frequency) and bring that data to a clinician visit specifically asking whether your presentation is joint-dominant and whether a TMJ injection plan—potentially including bpc-related protocols—is likely to match your pain generator.
Discussion