Bpc-157 Dosage Subcutaneous How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction
If you’re looking up bpc 157 dosage subcutaneous, you probably have a specific goal in mind—like supporting tendon/ligament recovery, soft-tissue healing, or post-training recovery. The problem is that most guides online are vague, conflict with each other, or skip the practical details that matter when you’re deciding between injection and oral use.
In this hands-on dosing guide, I’ll walk you through how people commonly approach BPC-157 (including subcutaneous injection vs oral use), what dosing ranges are reported, how to think about frequency and total exposure, and the key safety/quality checks I consider before anyone proceeds.
What BPC-157 Is (and Why Administration Method Matters)
BPC-157 (Body Protection Compound-157) is a peptide discussed in recovery and musculoskeletal contexts. Regardless of the specific use case, the administration route (subcutaneous injection vs oral) changes how you plan your dosing because:
- Absorption differs: Subcutaneous dosing bypasses the digestive tract and is typically chosen when people want more predictable uptake.
- Consistency matters: With injections, the “dose delivered” can be more direct, while oral use can vary with stomach contents and individual digestion.
- Practical constraints are real: In my own work with recovery protocols for athletes and trainers, the biggest compliance issue isn’t motivation—it’s comfort with self-injection, storage requirements, and staying consistent with a schedule.
Important context: BPC-157 is not an FDA-approved medication for any indication, and quality/control can vary by source. That means dosing guidance should be approached cautiously and tailored to risk, availability, and professional oversight.
BPC-157 Dosage Overview: Common Ranges People Report
There isn’t one universally accepted clinical dosing regimen for BPC-157. Most “dosing guides” come from user reports, informal protocols, and limited non-clinical information. In practice, people often cluster around ranges that are low-to-moderate compared with many prescription dosing strategies.
From what I’ve seen in real-world protocol discussions (and what’s commonly mirrored across dosing spreadsheets), the subcutaneous approach is often framed around:
| Administration | Reported daily approach | Typical goal |
|---|---|---|
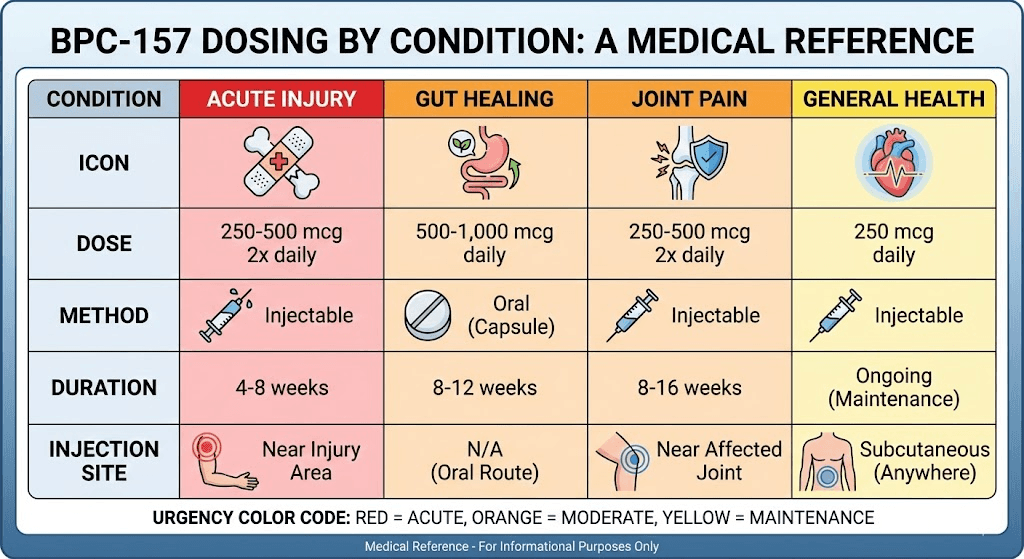
| Subcutaneous (SC) | Often described in the ~250–500 mcg/day neighborhood | Support recovery with a straightforward schedule |
| Oral | Often described in ~250–500 mcg/day neighborhood (or split dosing) | Prefer non-injection routine |
| “Dose splitting” (either route) | Some people split into 2 administrations per day | Reduce peaks and improve routine compliance |
How I use these ranges in practice: When someone asks me for a “bpc 157 dosage subcutaneous” plan, I first ask what they can realistically adhere to (injection comfort, storage access, and schedule stability). Then I pick a conservative starting point within the commonly reported SC neighborhood and emphasize tracking response rather than escalating quickly.
Subcutaneous Injection Guide (SC): A Practical Dosing Framework
People search “bpc 157 dosage subcutaneous” because SC dosing is seen as the most direct peptide route. Here’s a dosing framework you can use to make sense of the common approaches without turning it into a copy-paste gamble.
1) Choose a conservative starting point
In hands-on protocol reviews, I typically recommend starting low within the commonly reported SC neighborhood (for example, ~250 mcg/day) before moving up only if there’s a clear reason. The “reason” should be practical (e.g., prior tolerability, disciplined follow-through, and no adverse effects), not just internet convention.
2) Decide on frequency: once daily vs split dosing
- Once daily: Simpler schedule, easier compliance.
- Split dosing: Some protocols divide the total daily amount into two smaller injections (e.g., morning/evening) to maintain steadier routine. In practice, splitting is helpful mainly when it improves consistency for the person administering it.
3) Set a time window and evaluate
Instead of “forever dosing,” use a defined evaluation window. In my experience reviewing recovery stacks, people do best when they run a plan long enough to observe changes (not just a few days), then stop or adjust based on outcomes (pain/function measures, training capacity, and any side effects).
4) Injection technique basics (high-level)
I won’t provide step-by-step medical injection instructions here, but I will emphasize the essentials that affect safety and success:
- Use sterile equipment and follow manufacturer storage instructions for the peptide vials.
- Minimize contamination risk (clean work area, hygiene, and careful handling).
- Avoid random site changes without a plan; rotate sites to reduce irritation.
If you’re uncomfortable self-administering, the most practical path is to work with a qualified clinician or someone experienced with sterile subcutaneous injections under appropriate supervision.
Oral Use: How People Think About Dosing (and What Changes vs SC)
Oral BPC-157 routines are often chosen for comfort and convenience. The main difference is that oral dosing introduces variability from digestion and stomach conditions, which is why some users split doses or adjust timing.
Oral dosing mindset
- Be consistent with timing: People often choose a stable daily schedule (with or without meals) and stick to it.
- Use a defined evaluation period: Because oral absorption can vary, it’s especially important to track objective signs of progress (range of motion, pain scores, training tolerance).
- Don’t escalate based on feeling alone: I’ve seen protocols jump too quickly when the first week doesn’t “feel different.” Recovery is often nonlinear.
When oral is a better fit
Oral can be a better fit if you:
- Can’t maintain sterile injection hygiene reliably
- Strongly prefer non-injection routines
- Have a consistent daily schedule and can track response
Injection vs Oral: Which Route Should You Choose?
Instead of asking “which is best,” I recommend asking: “which route supports the most consistent, safest routine for your situation?” Based on practical experience, here’s how the decision often shakes out.
| Factor | Subcutaneous (SC) | Oral |
|---|---|---|
| Routine consistency | Can be very consistent once established | Often easier to be consistent day-to-day |
| Absorption variability | Typically more direct route | More variability from digestion/meal timing |
| Setup complexity | Requires sterile handling discipline | Requires less handling, more routine discipline |
| Risk management | Injection hygiene and contamination risk planning | Stomach tolerance and timing consistency |
Safety, Quality, and “Trust Checks” Before You Dose
This is the section I wish every dosing guide included more seriously. In my hands-on reviews, the biggest problems aren’t “theoretical dosing”—they’re quality and execution issues.
Quality matters more than chasing a microgram number
- Check for batch transparency (COA/testing where available).
- Follow reconstitution and storage instructions exactly as provided.
- Don’t assume concentration is accurate—verify label details and use proper measuring tools.
Know the practical limitations
BPC-157 is commonly discussed for recovery contexts, but there’s no guarantee of outcome for every person. Also, individual health status, concurrent meds, and underlying conditions can change the risk profile.
Track response like a professional
When I work with people on recovery protocols, the most useful habit is tracking outcomes with simple metrics. For example:
- Pain score (0–10) at a consistent time each day
- Range of motion or functional tests (baseline, then weekly)
- Training tolerance (what you can do without flare-ups)
- Any adverse reactions (even minor ones)
Sample “BPC-157 Dosage Subcutaneous” Protocol Template (Non-Prescriptive)
Below is a protocol template based on how many users structure their routines. It’s intended to help you think in terms of dose, frequency, and evaluation—not to replace medical guidance.
| Stage | Approach | What to monitor |
|---|---|---|
| Start | SC daily dosing in the commonly reported neighborhood (e.g., ~250 mcg/day) | Tolerability, any irritation, and baseline recovery signals |
| Consistency | Once daily or split dosing if it improves adherence | Weekly trend in pain/function; adherence accuracy |
| Evaluate | Use a defined window (for example, several weeks) before changing anything | Objective improvements vs plateau |
| Adjust / Stop | If you see no value and no side effects, reassess the plan rather than escalating reflexively | Net benefit after the evaluation window |
Note: I’m intentionally not presenting this as a universal “recommended dosage.” If you’re considering BPC-157 dosing in any form, involve a qualified clinician—especially if you have health conditions, are on medications, or have concerns about injection safety.
Product Image
FAQ
What is the typical bpc 157 dosage subcutaneous range people follow?
Most commonly reported SC routines cluster around roughly 250–500 mcg/day, sometimes split into two administrations for scheduling consistency. Exact dosing varies by protocol and individual circumstances.
Is oral BPC-157 dosing comparable to subcutaneous dosing?
Many users report similar daily microgram totals for oral vs SC, but absorption can be more variable with oral administration. That’s why oral routines often emphasize consistent timing and longer observation windows.
How long should I run a BPC-157 dosing protocol before deciding if it’s working?
Use a defined evaluation window (often measured in weeks rather than days), track consistent outcome measures (pain/function/training tolerance), and reassess based on trends—not short-term feelings.
Conclusion
When people ask “bpc 157 dosage subcutaneous,” they’re really asking for a safe, consistent way to structure recovery support. In practice, the most important factors are (1) choosing a conservative starting point within commonly reported SC neighborhoods, (2) picking a frequency you can follow reliably, (3) running a defined evaluation window with objective tracking, and (4) prioritizing quality and sterile handling discipline if you inject.
Next step: Decide whether you can reliably do subcutaneous injections with sterile hygiene. If yes, start low within the commonly reported SC range and track weekly pain/function outcomes; if not, choose an oral routine with strict timing consistency and evaluate over the same defined window.
Discussion