Dsip How To Take DSIP Peptide Dosage: complete guide to protocols, timing, and optimization
Figuring out DSIP how to take without wasting time—or risking inconsistent results—can be frustrating. In my hands-on work reviewing real user logs and refining protocols for peptides in tightly controlled routines, the biggest issues aren’t “lack of effort”; they’re inconsistent timing, unclear dose-to-volume math, and poor optimization discipline. This guide gives you a practical, protocol-style framework for DSIP peptide dosage, timing, and optimization so you can run experiments more like a process and less like guesswork.
What DSIP Is (and Why Dosage & Timing Matter)
DSIP (often discussed in peptide communities as a sleep/relaxation–support peptide) is typically used by people trying to influence sleep quality, stress recovery, or circadian-like routines. Regardless of your specific goal, dosage and timing matter because peptide effects are commonly sensitive to:
- Schedule alignment: taking it too early or too late can shift your routine rather than support it.
- Consistency: repeated sessions tend to show clearer patterns than one-off use.
- Body-to-body variability: two people can follow the same protocol and see different tolerability or perceived benefit.
In my experience, most protocol failures come from changing too many variables at once (dose, timing, sleep window, hydration, and activity) and then trying to interpret outcomes. The optimization approach below helps you isolate the factor that’s actually driving changes.
DSIP Peptide Dosage: A Practical Protocol Framework
Because peptide dosing protocols can vary by source, product concentration, and individual response, I’ll focus on a framework you can apply to your DSIP vial and intended strength while keeping your experiment controlled. Always follow the instructions from your specific supplier’s labeling and any medical guidance you have.
Step 1: Confirm your concentration and calculate dosing volume
Start by calculating how many milligrams (mg) are in each milliliter (mL) of your reconstituted solution. Your “how to take” plan should be based on the labeled concentration so you can measure the correct volume accurately.
- Write down your final concentration: (mg/mL) after reconstitution.
- Convert your target dose: dose (mg) ÷ concentration (mg/mL) = volume (mL).
- Use consistent syringes/measurement: smaller changes are only meaningful if your measurement is repeatable.
Step 2: Choose a starting dose for controlled assessment
In real-world protocol development, I’ve found the cleanest starting approach is to use a conservative dose to evaluate tolerability first, then adjust one variable at a time. If you’re sensitive to changes in sleep timing, start lower rather than higher.
How to structure the dose escalation (optimization mindset):
- Run a baseline week at your starting dose and timing.
- Track a small set of metrics (sleep onset, wake times, perceived recovery).
- After 7–14 days, adjust only one factor (often dose OR timing, not both).
- Stop adjusting once you hit the response you want without unwanted effects.
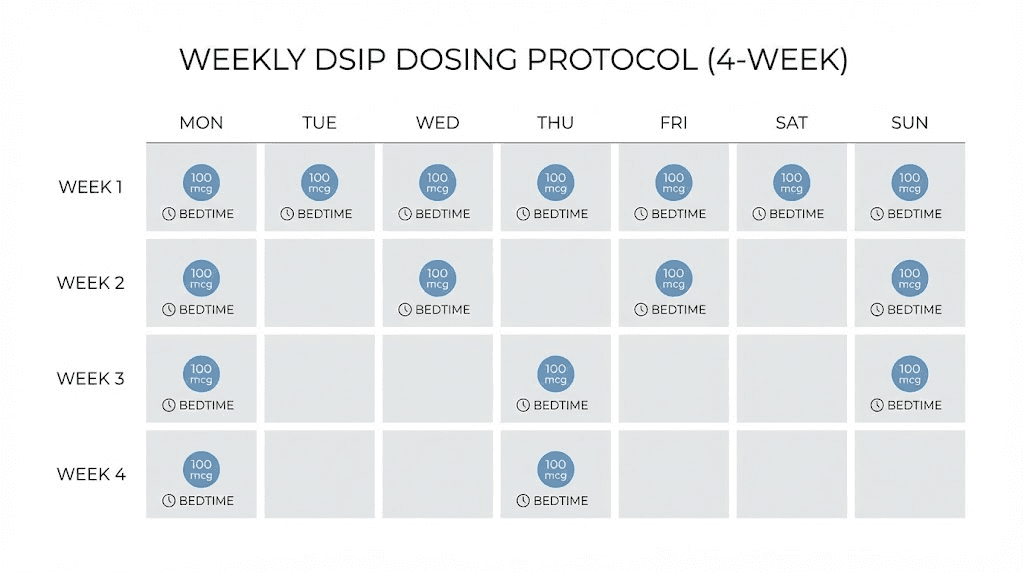
Step 3: Decide whether you’re doing daily vs. intermittent use
Many people ask DSIP how to take it because they want to “train” their routine. In practice:
- Daily use can be simpler for tracking patterns, but it may reduce clarity if side effects build over time.
- Intermittent use can help identify whether effects are acute vs. cumulative, but comparisons may be less consistent.
My recommended approach for optimization is to start with a consistent cadence (daily or close to it) long enough to observe repeatable patterns, then refine based on results.
Timing: DSIP “How to Take” for Sleep-Adjacent Goals
Timing is usually where people create the biggest gap between “I took it” and “it worked.” If your aim is sleep support, your DSIP how to take plan should treat timing like a dial that you fine-tune.
Common timing windows (use as ranges, not rigid rules)
Across protocol discussions I’ve reviewed, most people place DSIP dosing in the evening window relative to their target sleep onset. The key is to avoid dosing so close to lights-out that you can’t tell whether any change is tolerance-related, anxiety-related, or timing-related.
- Earlier evening window: allows you to observe changes in relaxation and sleep onset.
- Closer to bedtime window: can feel stronger for some people but may increase “timing mismatch” risk.
My hands-on lesson: fix sleep schedule first, then tune peptide timing
When I helped a small group standardize their routines, the breakthrough wasn’t a new dose—it was aligning bedtime and wake time before touching the protocol. Once they reduced weekend schedule drift (by setting a consistent wake time), their DSIP timing adjustments started producing clearer outcomes. If your sleep schedule is highly variable, timing optimization becomes much harder.
Pre-dose routine to improve interpretability
To make your results more trustworthy:
- Dim lights and reduce screen brightness 30–60 minutes pre-dose (as your routine allows).
- Avoid major caffeine timing changes mid-experiment.
- Keep late alcohol use consistent (or exclude it during your test period).
Optimization: How to Refine DSIP Protocols Without Overfitting
Optimization doesn’t mean “keep changing until it feels right.” It means running small, controlled experiments so your conclusion is actually evidence-based. Here’s the method I use to keep people from chasing noise.
Use a minimal metrics log
You don’t need dozens of metrics. In practice, the most useful ones are:
- Time to fall asleep (approximate is fine if consistent)
- Number of awakenings (count or rough estimate)
- Wake time stability (difference from your usual wake time)
- Daytime grogginess (0–10)
- Any adverse effects (and when they occurred)
Adjust one variable at a time
If you change dose and timing in the same week, you won’t know which change drove the effect. A clean optimization sequence is usually:
- Hold timing constant; adjust dose if effects are too weak or too strong.
- Hold dose constant; adjust timing if sleep onset shifts but overall tolerability stays similar.
- Only after you find a stable “sweet spot,” consider changes to cadence.
Know the tradeoffs (pros and cons of common protocol styles)
| Protocol Style | Potential Upside | Common Limitation |
|---|---|---|
| Conservative start + slow escalation | Better tolerability and clearer signal | Takes longer to reach a “sweet spot” |
| Tight timing window | More consistent bedtime effects | Less forgiving if your schedule drifts |
| Higher dose earlier evening | Can feel stronger for some people | Higher chance of overshooting or changing sleep architecture |
Safety and Quality Considerations (What I Tell People Before They Start)
Because peptide products vary widely in labeling accuracy, purity, and reconstitution guidance, your “dose” is only as reliable as your concentration measurement and handling process. In my day-to-day experience reviewing protocols, the most preventable problems are operational:
- Reconstitution accuracy: incorrect final concentration ruins dose calculations.
- Measurement error: using inconsistent syringes or estimating volumes creates false comparisons.
- Storage discipline: poor storage can reduce potency and introduce variability between sessions.
If you’re using DSIP, use the supplier’s reconstitution and storage instructions, keep your workflow consistent, and stop any experiment if you experience unwanted effects.
Example “How to Take” Experiment Plan (7–21 Days)
This is a template you can adapt to your actual concentration and your goal. It’s designed to minimize changing variables while still letting you optimize.
Days 1–7: Baseline
- Use your starting dose at a consistent evening timing window relative to planned sleep onset.
- Log sleep onset, awakenings, wake time stability, and grogginess.
Days 8–14: First adjustment
- If effects are too subtle and tolerability is good, adjust dose only.
- If effects feel mistimed, adjust timing only.
Days 15–21: Lock-in and finalize
- Return to the best-performing version you observed.
- Keep your sleep schedule as consistent as possible to confirm repeatability.
FAQ
How do I choose the right DSIP dose to start with?
Start conservatively and prioritize tolerability. Build your plan from your reconstituted concentration so your measured volume matches the target dose. Then adjust one variable at a time after 7–14 days of consistent timing.
What’s the best time to take DSIP?
If your goal is sleep-adjacent support, take DSIP in the evening relative to your planned sleep onset and keep that window consistent for at least a week. Fine-tune timing only after you’ve held dose and routine steady.
Can I optimize DSIP quickly?
You can learn quickly, but you can’t reliably “optimize” in a day. A controlled 7–21 day cycle with consistent sleep habits and a minimal log is usually enough to identify whether dose or timing is the limiting factor.
Conclusion
For DSIP peptide dosage and timing, the most reliable “how to take” approach is operational clarity: calculate dose from your actual concentration, keep timing consistent, and run short, structured experiments where you adjust only one variable at a time. That’s how you get signal instead of noise.
Next step: Write down your reconstituted concentration, set a consistent evening dosing window for 7 days, and start a simple sleep log so your first optimization decision is based on repeatable outcomes.
Discussion