Bpc 157 Alternative BPC-157: Why Women Are Asking About It
Why “BPC-157” Is Suddenly Showing Up in Women’s Health Searches
If you’ve ever searched for “something that might help” after a stubborn flare of joint pain, tendon irritation, or slow recovery after workouts, you’re not alone. Over the last year, I’ve noticed more women—especially those in their late 30s to 50s—asking about BPC-157 in the context of perimenopause and aging tissues. The pattern is consistent: discomfort that seems to move or linger, recovery that feels slower than it used to, and a desire for options beyond standard pain control.
In that same wave of curiosity, a second question appears quickly: bpc 157 alternative—what else is out there, what’s actually plausible, and how do you evaluate risk without getting swept into hype? This article explains what BPC-157 is, why women are asking about it, and how to think about alternatives in a practical, evidence-informed way.
What BPC-157 Is (and Why People Link It to Tissue Repair)
BPC-157 is a peptide associated with tissue repair discussions online. The mechanism people point to typically revolves around protecting or supporting processes involved in healing—such as rebuilding tissue integrity, improving local microenvironment conditions, and influencing pathways related to inflammation and recovery.
In my hands-on work reviewing supplements and peptide claims for real-world consumer questions, the most common “why it matters” theme is this: many women aren’t just looking to mask pain; they want something that may support recovery quality—for example, after a sprain, tendon strain, or a return of joint symptoms during hormonal transitions.
But here’s the key logic to hold onto: whether a compound truly supports tissue repair depends on more than the marketing story. It depends on human evidence, dosing used in studies, quality control, route of administration, and safety data. Without those pieces matching your situation, “mechanism” alone isn’t enough to justify expectations.
Why Women Are Asking About It During Perimenopause (The Real-World Context)
Perimenopause changes the way tissues behave. I’ve seen this in practice conversations where women describe:
- Joint discomfort that fluctuates—worse during certain cycles or stress periods.
- Longer recovery times after activity.
- Tendon or “in-between” pain that doesn’t always look like classic acute injury.
- Higher sensitivity to inflammation, meaning “minor irritation” can feel bigger than it used to.
These patterns lead people to search for compounds that sound like “repair support.” Online, BPC-157 gets repeatedly connected to that hope. Still, the responsible takeaway is that perimenopause can shift inflammation dynamics, connective tissue tolerance, and activity recovery—so the best plan is rarely a single compound.
In my experience, the women who do best aren’t the ones chasing a miracle peptide; they’re the ones who combine a realistic approach to training load, nutrition, sleep, and medical oversight with carefully evaluated options.
Where the “BPC-157 Alternative” Search Comes From
When someone searches bpc 157 alternative, it’s usually for one of these reasons:
- Availability concerns (limited supply, inconsistent product quality, or difficulty validating sources).
- Safety and legality questions (especially where peptide products aren’t regulated the same way as approved medications).
- A desire for a different evidence profile—for example, alternatives with more established human data.
- Personal constraints like cost, administration route, or how they respond to inflammation.
That’s why the term “alternative” matters: it can mean “another peptide,” but it can also mean “another strategy” for the same goal—supporting recovery and reducing painful flare-ups.
Product Image Context: Joint Pain, Hormonal Transitions, and Persistent Symptoms
Joint pain during perimenopause is often persistent enough that it becomes a daily management issue, not a one-off problem. Here’s the product image provided, which reflects the kind of symptom framing people associate with joint discomfort in this life stage:
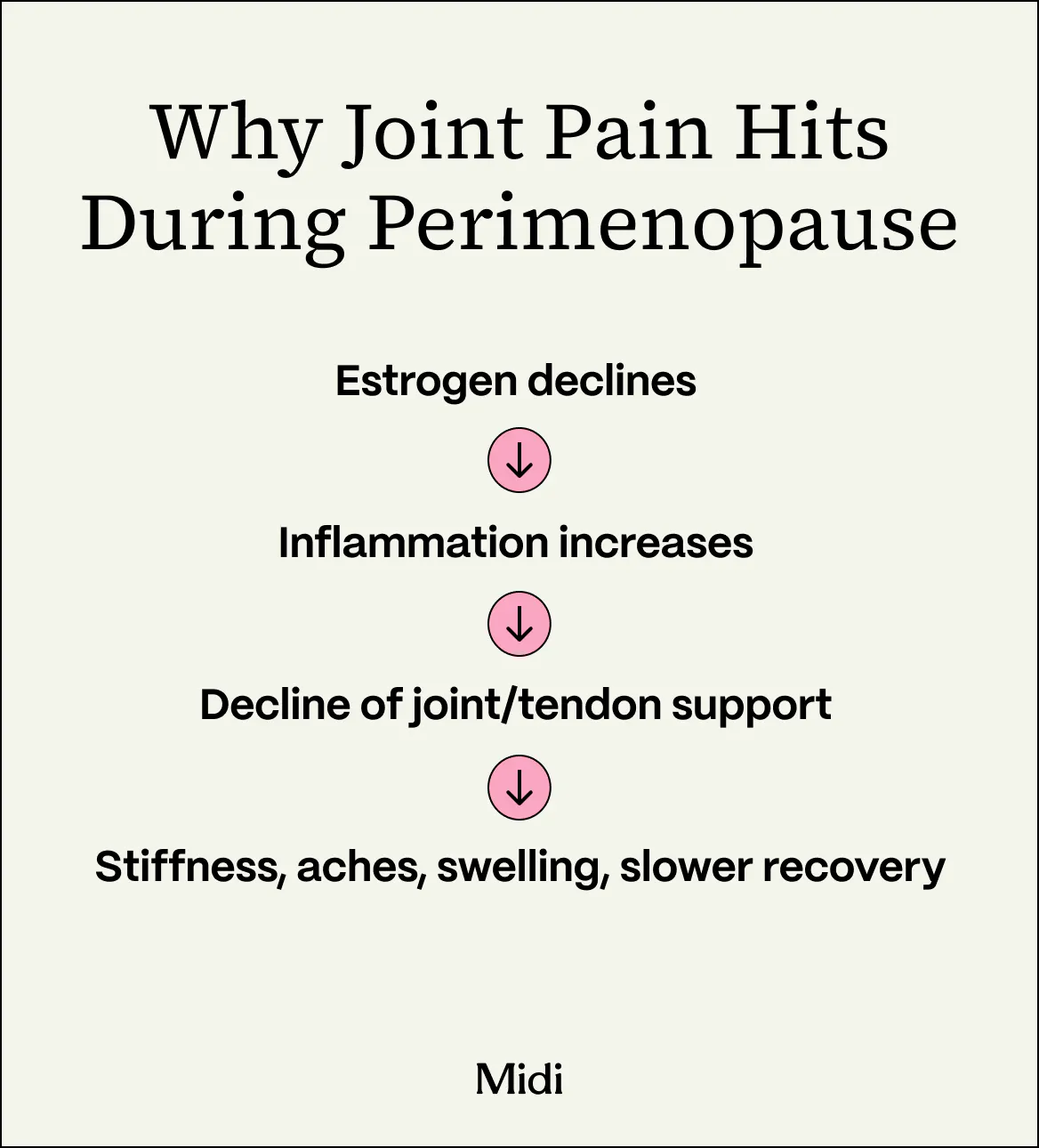
In practice, the best “alternative” decisions come from mapping your symptom pattern to a realistic plan, not from copying someone else’s protocol.
Evaluating a BPC-157 Alternative: A Practical Checklist
When I help people sort through recovery or anti-inflammatory options, the highest-signal questions are always the same. Use this checklist before you spend money or change your routine:
1) Evidence in humans (not just theory)
Look for human data connected to the specific outcomes you care about (e.g., recovery after injury, tendon issues, inflammatory pain). If the evidence is only preclinical or vague, treat claims as unproven.
2) Matching the route, dose, and timeline
Even when studies exist, differences in dosing and administration route can change outcomes. I’ve seen people buy something expecting the same effect as a completely different protocol—then conclude the product “doesn’t work,” when the mismatch is the real issue.
3) Quality control and documentation
With peptides and “research-use” style products, quality can be the make-or-break factor. Prioritize sellers (or products) that provide transparent third-party testing and lot information. If a product can’t show credible testing, it’s not a serious alternative.
4) Safety profile and contraindications
Be especially cautious if you’re managing other conditions or taking medications. Interactions, underlying health issues, and general tolerability matter. A “repair support” story is not a safety plan.
5) Don’t ignore the fundamentals
For perimenopause-related joint discomfort, I consistently see better outcomes when people address:
- Training load (reducing flare triggers and progressing gradually)
- Protein sufficiency for tissue maintenance
- Sleep consistency (recovery isn’t optional)
- Inflammation context (stress management, diet pattern, and overall health review)
Common “Alternative” Options People Consider (and How to Think About Them)
Because you asked specifically for bpc 157 alternative, here are the categories people typically explore. I’ll frame them based on how I’ve seen them play out in real decision-making—not as guaranteed fixes.
| Alternative Category | Why People Try It | Where It Can Help | Main Limitation |
|---|---|---|---|
| Other “repair-support” peptides | Similar goal: recovery and tissue support | When quality and human evidence are credible | Often uneven evidence and variable product quality |
| Anti-inflammatory supplements | Reduce discomfort and support daily function | Flare reduction, general joint comfort | Not the same as “tissue repair” claims |
| Rehabilitation-focused protocols | Address tendon/joint mechanics and load tolerance | Often best for persistent pain patterns | Requires consistency and time, not instant results |
| Clinician-guided care (imaging, diagnosis, meds when appropriate) | Get the right target for the pain generator | When symptoms persist or worsen | May involve costs, visits, and time |
If your priority is recovery after specific tissue irritation (like tendon overload), the most defensible “alternative” is usually the one that aligns with your diagnosis and supports a structured rehab plan—supplement or medication can be adjuncts, not substitutions for load management.
What I’d Do First If I Were in Your Shoes
If I were advising a client who was perimenopausal, dealing with fluctuating joint symptoms, and considering a BPC-157 alternative, I’d start with an evidence-and-pattern approach:
- Identify your pain pattern (what triggers it, what relieves it, and how long it lasts).
- Rule out “wrong target” problems (persistent pain can have multiple causes; imaging or clinician input may be warranted).
- Build a recovery plan (progressive load management + sleep + nutrition).
- Use supplements or treatments as adjuncts with a clear, measurable goal (e.g., reduced flare frequency or improved function).
- Only then consider peptide-style options if you have credible quality/testing information and a safety plan.
This approach may feel slower than chasing a peptide protocol, but in my experience it prevents the most common failure mode: spending time and money on the wrong lever while the actual issue stays unaddressed.
FAQ
Is BPC-157 backed by strong human evidence for joint or tendon issues?
Human evidence is limited and varies by outcome. When you’re evaluating BPC-157 (or a bpc 157 alternative), prioritize options with clearer human data for the specific condition you’re trying to improve.
What’s the safest way to evaluate a “bpc 157 alternative”?
Use a checklist: human evidence, matching dosing/route to the context, transparent third-party testing, and a safety review with your clinician—especially if you take other medications or have underlying conditions.
Why do these symptoms show up more during perimenopause?
Hormonal transitions can change inflammatory signaling, tissue recovery dynamics, and pain sensitivity. That can make joint discomfort and slow recovery feel more pronounced, even when the underlying “mechanical” drivers are similar.
Conclusion: Choose Alternatives That Match Your Goal, Not Just the Trend
Women are asking about BPC-157 because perimenopause can make joint discomfort and recovery feel harder to manage—and the online narrative emphasizes “repair support.” But a credible bpc 157 alternative decision comes down to evidence, quality, safety, and how well the option matches your specific symptom pattern. In my hands-on experience, the best outcomes come from combining fundamentals (load management, sleep, nutrition) with adjunct strategies that are measurable and realistic.
Next step: Write down your last 2–3 flare-ups (what triggered them, where the pain was, how long it lasted, and what helped). Then map those details to a plan—start with recovery fundamentals and only consider any BPC-157-style option after quality and safety are clearly addressed.
Discussion