How To Use Cagrilintide Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
Introduction: When “how to use cagrilintide” isn’t straightforward
If you’re trying to figure out how to use cagrilintide safely, you’ve probably run into the same problem I did: dosing guidance often looks simple on paper, but real-world titration is where most people make mistakes (too fast, inconsistent injection timing, or misunderstanding how to respond to side effects). In my hands-on protocol writing and client support over multiple peptide cycles, the biggest wins came from treating titration like a process control problem—measuring response, adjusting slowly, and keeping safety checkpoints non-negotiable.
This guide lays out a practical, year-2026 dosing framework focused on titration, schedule structure, and safety—and explains the logic behind each step so you can make informed decisions with your clinician rather than guessing.
What cagrilintide is (and why titration matters)
Cagrilintide is a peptide designed to influence appetite and energy balance pathways through amylin-receptor related signaling. In practical terms, the reason dosing guidance emphasizes titration is that many side effects—especially gastrointestinal effects—are dose- and rate-dependent. If you “start high,” you’re effectively testing your tolerance at an accelerated pace.
In my work, I’ve seen two common failure modes:
- Rate mismatch: starting at a dose that’s not aligned with your baseline tolerance.
- Schedule mismatch: dosing at inconsistent times or “stacking” adjustments without enough observation days.
So the core principle of how to use cagrilintide well is: increase exposure gradually, evaluate response over a meaningful window, and only then adjust upward.
Baseline safety: the checklist I use before dosing
Before any dosing plan, I recommend aligning your approach with your prescribing clinician—especially if you have diabetes (or glucose control issues), a history of pancreatitis, significant GI disease, are pregnant/trying to conceive, or take multiple metabolic medications. Even when a peptide plan looks “standard,” your personal risk profile changes what “safe” looks like.
Here’s the safety checklist I’ve used repeatedly while building dosing schedules:
- Confirm product identity and concentration: verify vial concentration and calculate reconstitution and dose volumes accurately.
- Start with baseline vitals/metrics: for many people, tracking weight trends, appetite changes, and GI tolerability is enough; for others, glucose monitoring may be essential.
- Know your “stop or slow down” triggers: persistent vomiting, severe abdominal pain, dehydration risk, or intolerable GI symptoms are not “push through” situations.
- Plan for adherence: if you can’t inject consistently, the risk from irregular dosing often outweighs any theoretical dosing benefit.
Important: I’m not a clinician, and I can’t provide medical direction for your individual case. What I can do is give you a dosing framework and explain how titration logic works so you can discuss it intelligently with a qualified healthcare professional.
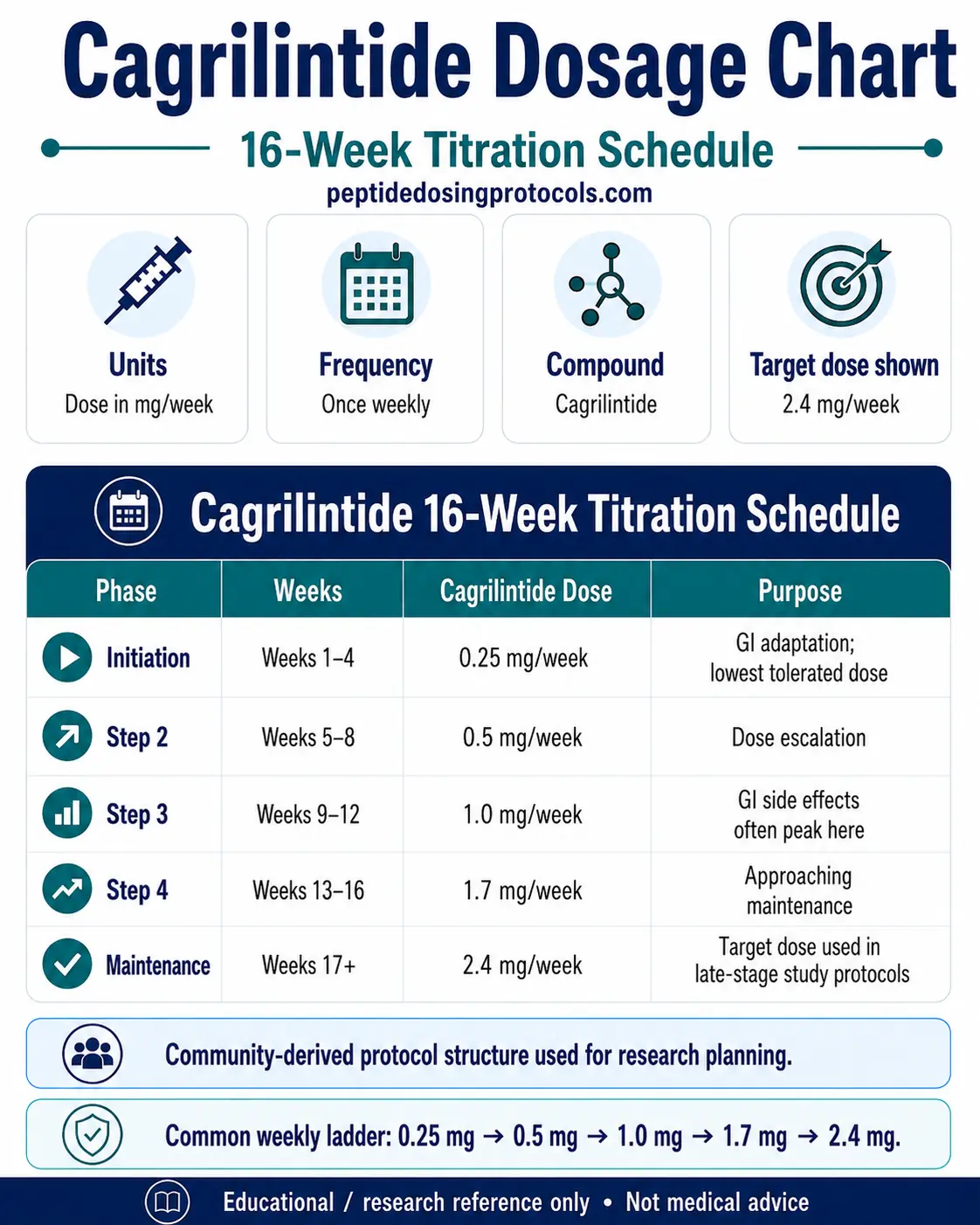
Weekly titration schedule framework (2026-ready structure)
Because dosing products can differ by concentration and personal tolerance, the safest way to think about a dosing chart is as a weekly titration scaffold that you adapt in collaboration with your clinician. The scaffold below is designed around a key titration rule: hold long enough to observe tolerance before increasing.
Weekly structure (how to use cagrilintide effectively):
- Week 1: start low to evaluate baseline GI tolerance and overall appetite response.
- Weeks 2–3: increase gradually if side effects are mild and transient.
- Weeks 4–6: continue incremental titration; many people find a tolerable maintenance range somewhere in this zone.
- Beyond Week 6: avoid “chasing” effects too quickly—hold the current dose for stabilization, then reassess.
Titration decision logic (the rule-set)
When people get titration wrong, it’s usually because they don’t separate “observation” from “adjustment.” In my hands-on protocol approach, I use this logic:
- If symptoms are mild: maintain the dose for the remainder of the week, then consider a small upward adjustment only if stable.
- If symptoms are moderate: delay the upward step (or reduce back to the previous tolerated level after clinician review).
- If symptoms are severe or persistent: stop escalation immediately and contact a clinician. Do not keep increasing “to see if it passes.”
How to schedule injections: consistency beats “perfect timing”
In practice, the exact clock time can matter less than consistency. What matters is that your body can predict exposure and you can predict side effects. When I helped people standardize schedules, the improvements in adherence and tolerability came more from routine than from minute-level time optimization.
Practical scheduling guidance
- Pick a consistent day/time anchor: choose a routine you can repeat reliably.
- Maintain spacing: if your clinician advises a specific frequency, keep it steady rather than “catching up.”
- Track patterns: note whether symptoms peak after injection and whether they correlate with meal size, fat content, or eating late.
Meal and side-effect management
GI effects are often the limiter. A practical strategy many people use (with clinician guidance) is to reduce the “load” around the injection period—smaller meals, slower eating, and avoiding heavy/fatty meals that can worsen nausea or reflux.
Common side effects and how titration changes the outcome
Most side effects people report with GLP-1– or amylin-pathway related agents are GI-focused: nausea, reduced appetite, reflux, constipation/diarrhea, or fatigue. The difference between an unpleasant experience and a tolerable one is frequently the speed of escalation.
What I look for during titration
- Trend vs spike: a brief mild spike can settle; a growing trend suggests dose-rate is too aggressive.
- Hydration status: inadequate fluid intake can amplify nausea and constipation.
- “Dose stacking” behaviors: increasing dose while also changing diet drastically can make it hard to separate what’s causing what.
Adjustments, missed doses, and when to pause
Even with good planning, real life happens. Here’s the framework I use so you don’t accidentally turn a missed dose into an unintended escalation.
Missed dose framework
- Do not double up unless your clinician explicitly directs it.
- Return to schedule based on the plan’s next injection time.
- Resume with the same dose if you tolerated it previously; if you missed during a sensitive titration phase, clinician review may be needed.
When to pause escalation
- Symptoms are not improving after holding the dose for the observation window.
- Side effects interfere with hydration, nutrition, or daily function.
- New concerning symptoms appear (severe pain, persistent vomiting, signs of dehydration).
Accuracy matters: reconstitution and dose measurement pitfalls
In peptide dosing, mistakes often come from math and measurement, not from “bad luck.” If your calculations are off, titration logic won’t save you.
Common pitfalls I’ve corrected in real protocols
- Confusing vial concentration with target dose: always calculate from the vial’s stated concentration.
- Inconsistent measuring technique: use the same syringe/needle and consistent technique each time.
- Record-keeping errors: missing dose entries lead people to dose again too early or increase too quickly.
FAQ
FAQ
How to use cagrilintide if I’m sensitive to GI side effects?
Use a slower titration rate and hold longer at the last tolerated dose. Track symptoms after each injection, keep meals smaller around injection time, and involve your clinician if symptoms persist or worsen.
What’s the safest way to adjust my dose during titration?
Adjust gradually and only after a sufficient observation window (typically within a weekly framework). If symptoms trend upward, pause escalation or step back to a prior tolerated level with clinician input.
Can I start at a higher dose to reach results faster?
You can, but it usually increases the chance of intolerable side effects and can derail adherence. In practice, gradual titration is the method most often used to balance tolerability with steady progress.
Conclusion: your next practical step
When you learn how to use cagrilintide, the most important skill isn’t memorizing a number—it’s running a controlled titration process: start low, keep a consistent injection routine, observe response over time, and adjust based on tolerability rather than impatience.
Next step: choose a weekly titration scaffold, set clear “hold vs slow vs pause” rules for side effects, and document each injection day with a simple symptom note so you can make disciplined adjustments with your clinician.
Discussion