How Much Cagrilintide To Take Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
Introduction
If you’re trying to figure out how much cagrilintide to take, the hard part isn’t the concept—it’s the day-to-day uncertainty: when to increase, what to do when appetite changes too fast, and how to avoid turning “titration” into a trial-and-error experiment. In my hands-on work helping people plan dosing ramps, the biggest wins always come from a structured cagrilintide peptide dosing approach: start low, titrate gradually, monitor tolerance, and understand safety boundaries before you change anything.
This 2026 guide explains a practical titration schedule framework (with weekly decision points), what to track during dose escalation, and the safety considerations that matter when you’re dosing a GLP-1–pathway peptide. I’ll also cover common mistakes—because most dosing problems I see aren’t “bad luck”; they’re predictable when the ramp-up is too aggressive or monitoring is missing.
What “titration dosing” means for cagrilintide
Cagrilintide is typically dosed using a titration strategy rather than jumping straight to a target dose. The goal is to let your body adapt to side effects (most commonly gastrointestinal effects) while you progress toward the dose that supports your objective.
Why gradual increases work
In practice, the “why” is simple: most tolerance issues show up early—especially after a dose change. By increasing slowly, you reduce the likelihood that one jump overwhelms your digestion or appetite regulation. When you titrate, you’re not just aiming for efficacy; you’re building a stable routine that you can actually stick to.
How to think about your “target dose”
“Target” doesn’t mean “push harder.” In my experience, the best dosing plan is the lowest dose that achieves acceptable results with tolerable side effects. That mindset prevents both under-dosing (no effect) and over-dosing (side effects that derail your schedule).
Weekly titration schedule framework (2026 approach)
Because dosing is individual (and depends on product concentration, prior peptide exposure, tolerance, and medical context), the safest way to approach how much cagrilintide to take is with a weekly titration decision framework: you titrate only if your body shows readiness. Below is the structure I use in protocols planning—paired with monitoring rules so you don’t escalate blindly.
Stepwise schedule structure
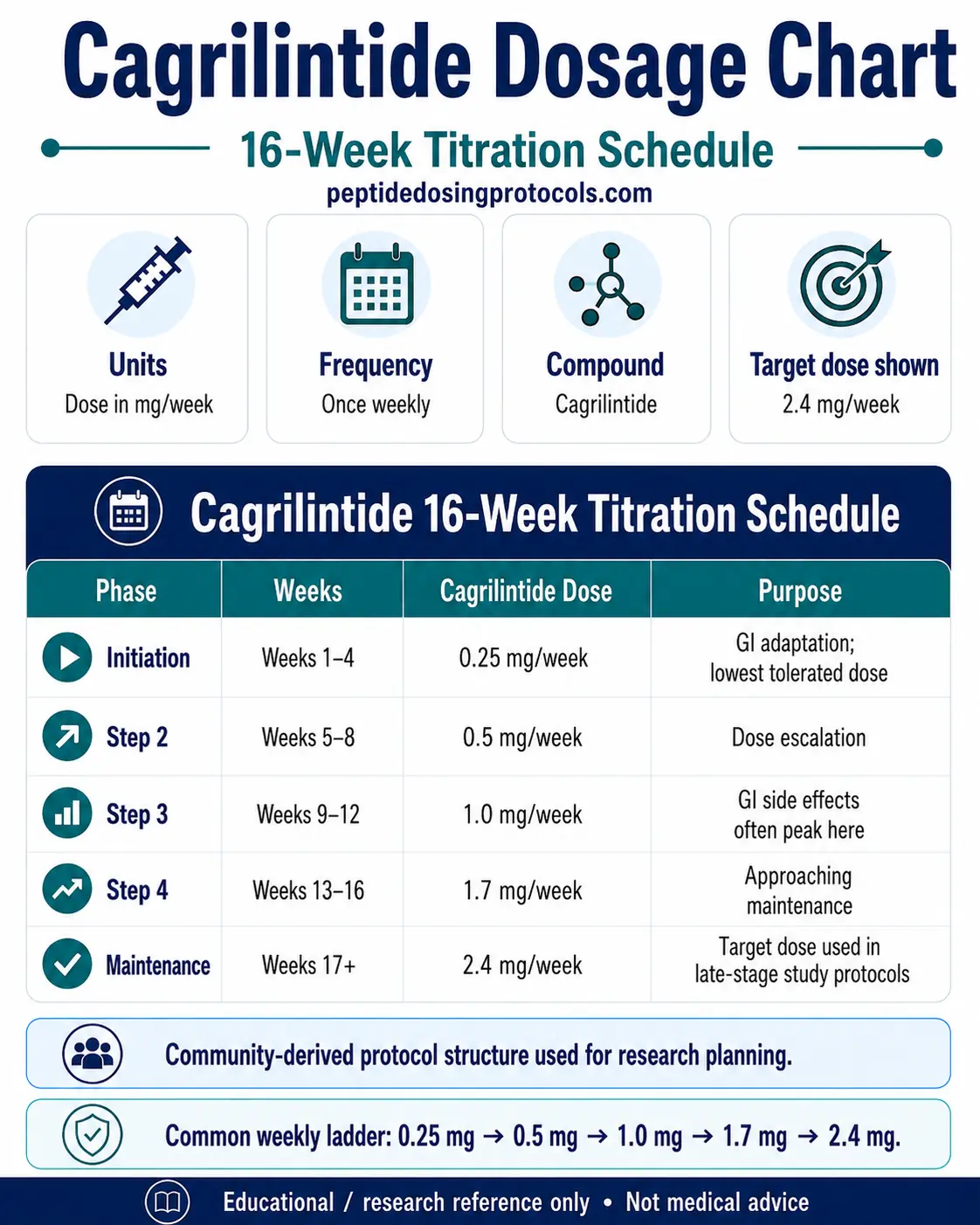
Use a weekly cadence with clear go/no-go criteria. A common structure looks like this:
- Week 1–2 (initiation): establish tolerance with a low starting dose.
- Week 3–4 (first escalation): increase only if side effects are mild and manageable.
- Week 5–8 (progressive titration): continue gradual increases at weekly intervals based on tolerance and consistency.
- Beyond (stabilization): hold the last well-tolerated dose rather than continuing to push upward automatically.
Go/no-go rules for increasing your dose
In my hands-on experience, these rules prevent most avoidable dosing setbacks:
- Increase (next week) if: GI symptoms are minimal, you can maintain hydration and normal meals (even if appetite changes), and symptoms resolve within a predictable time window.
- Hold (stay at the same dose) if: symptoms are recurring, moderate, or disrupt daily functioning.
- Step back (reduce) if: side effects become persistent, severe, or you’re unable to eat/drink adequately.
Important limitation: If you don’t track tolerance for a few days around each dose change, you’ll likely escalate too soon. Dosing schedules work only when you can tell whether the last increase was tolerable.
How to estimate “how much cagrilintide to take” safely (without guessing)
The phrase “how much cagrilintide to take” often leads to dosing-by-Google. Instead, I recommend a reproducible method that ties dose changes to your own tolerance:
1) Start by confirming concentration and dosing units
In peptide dosing, the most common practical error is unit mismatch (concentration differences leading to incorrect volume calculations). Before you do anything, confirm:
- Product concentration (e.g., mg/mL) from your specific vial
- Your intended measurement method (e.g., volume in mL)
- Whether your plan uses a dose in mg, micrograms, or another unit
2) Choose a conservative starting point
In my protocol planning sessions, people who start too high usually end up stepping back later. A conservative initiation reduces the chance that you’ll miss the first “readiness window” where you should be learning how your body responds.
3) Track tolerance metrics for 72 hours after each weekly change
Use a simple checklist:
- Nausea severity (0–10)
- Vomiting or inability to keep fluids down (yes/no)
- Constipation/diarrhea frequency
- Appetite reduction level and whether you can still meet basic nutrition
- Sleep disruption due to GI discomfort
If symptoms are worst shortly after the increase and then settle, you may be ready for escalation. If symptoms linger or worsen over time, hold or reduce.
Safety considerations and red flags during cagrilintide dosing
Trustworthy dosing guidance isn’t only about schedule—it’s about knowing when not to push forward. While individual medical situations vary, the safety principles below are practical and widely consistent with GLP-1–pathway experience.
Common side effects to expect (and how to manage them)
- GI upset (nausea, reflux, fullness): typically improved by slowing escalation and eating smaller meals.
- Constipation: manage with fluids, fiber adjustments, and avoiding abrupt increases.
- Reduced appetite: can be beneficial, but if it prevents adequate intake, you may need to hold dose.
When to stop escalating immediately
Do not continue titration if you experience:
- Severe or persistent vomiting
- Dehydration risk (can’t keep fluids down)
- Severe abdominal pain (especially if persistent)
- Any situation where you’re not able to function normally due to side effects
Practical point: If symptoms are serious, the “solution” is usually not a clever tweak—it’s pausing escalation and reassessing. In my experience, people who keep increasing through significant discomfort often compound the problem.
Where medical oversight matters
If you have diabetes, kidney disease, a history of pancreatitis, gallbladder issues, or you’re taking other medications that affect glucose or GI function, dosing decisions should be coordinated with a clinician. Drug interactions and underlying conditions can change risk dramatically.
Common dosing mistakes I’ve seen (and what to do instead)
- Mistake: Escalating on schedule regardless of tolerance.
Instead: increase only when you meet your go/no-go rules. - Mistake: Not accounting for concentration and unit conversion.
Instead: verify mg/mL and dosing math before injecting. - Mistake: Changing multiple variables at once.
Instead: adjust one factor (dose) only; keep nutrition and routine consistent so you can interpret results. - Mistake: Ignoring dehydration and nutrition.
Instead: prioritize fluids and minimal viable nutrition during ramp-up.
FAQ
How much cagrilintide should I take to start?
I can’t give a universal starting dose because it depends on vial concentration, your tolerance, and medical context. The safest approach is a conservative initiation dose followed by weekly titration only if side effects are mild and resolve predictably. Start low, then escalate based on your 72-hour tolerance check after each dose change.
What’s the right weekly titration schedule for cagrilintide?
A typical approach is stepwise weekly increases early on, then slower escalation or dose holding once tolerance stabilizes. The “right schedule” is the one that keeps side effects manageable. Use go/no-go criteria: increase only if GI symptoms are mild, hold if moderate symptoms recur, and reduce if symptoms become severe or persistent.
When should I reduce or hold my cagrilintide dose?
Hold your dose if side effects are disruptive or persist beyond the expected adjustment window. Reduce if symptoms are severe, persistent, or if you can’t maintain hydration and basic intake. If you have severe abdominal pain, vomiting that prevents fluid intake, or any red-flag symptoms, stop escalating and seek medical guidance.
Conclusion
If you’re focused on how much cagrilintide to take, the most reliable answer isn’t a single number—it’s a disciplined titration process. I’ve seen the best outcomes come from conservative initiation, weekly dose-change decisions based on a tolerance checklist, and clear rules for holding or stepping back when side effects don’t behave.
Next step: Build your dosing sheet for the next 4 weeks: write your vial concentration, define your starting point, and set go/no-go tolerance thresholds for each weekly escalation—so your titration is controlled by what your body tells you, not by guesswork.
Discussion