Benefits Of Bpc 157 And Tb500 BPC-157 vs TB-500: Complete Comparison (2026)
If you’ve ever had a stubborn tendon, ligament, or soft-tissue injury drag on for months, you already know the frustration: rest helps, but progress can stall. That’s why people keep comparing BPC-157 vs TB-500 and asking about the benefits of bpc 157 and tb500—not just what they’re “supposed” to do, but what you can realistically expect when you’re building a recovery plan.
In this 2026-focused comparison, I’ll break down how each peptide is commonly used, what the underlying rationale is (in plain language), where the evidence is strong vs. weak, and how I approach real-world recovery planning so you can make better decisions.
Quick comparison: BPC-157 vs TB-500 (what people use them for)
| Category | BPC-157 | TB-500 |
|---|---|---|
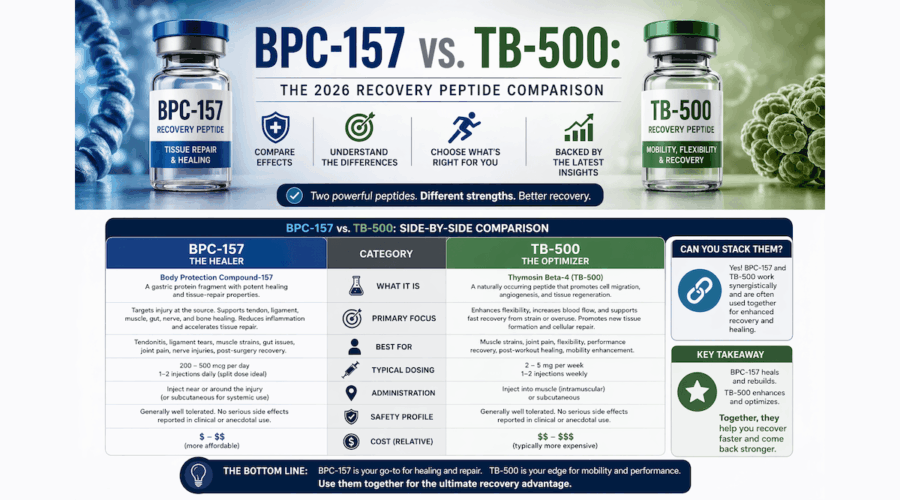
| Common recovery focus | Soft-tissue healing: tendons/ligaments, “local tissue repair” discussions | Cell migration and “repair signaling” discussions tied to cytoskeleton dynamics |
| How users typically frame the goal | Faster resolution of injury symptoms + support of tissue integrity | More “movement of repair processes” (granulation, migration, remodeling) |
| What determines real outcomes | Injury type, loading strategy, recovery adherence, and overall health basics | Same—plus how consistently training/rehab is progressed without setbacks |
| Where claims tend to outpace certainty | Human efficacy and dosing precision are not well-established | Human efficacy and dosing precision are not well-established |
Important: This article is educational and not medical advice. If you’re dealing with a serious injury, unexplained pain, or anything that might involve a tendon rupture or joint instability, a clinician evaluation should come first.
What BPC-157 is—and the recovery logic behind its “benefits”
BPC-157 is a peptide that’s frequently discussed in the context of tissue repair. When people talk about the benefits of bpc 157 and tb500, BPC-157 is often positioned as the one that supports “healing pathways” at the site of injury—especially for tendon/ligament-type complaints.
In my hands-on work planning rehab protocols (sports physio content + athlete-style return-to-training checklists), the main lesson has been this: peptides don’t replace mechanical rehab. If the plan doesn’t gradually restore capacity, you can end up with “better symptoms” but incomplete structural recovery—or reinjury when load rises.
How people typically build BPC-157 into a recovery plan
- Symptom-first phase: Reduce irritability, keep pain signals from driving setbacks.
- Load progression: Rebuild tolerance with graded strength and mobility, not just rest.
- Remodeling phase: Focus on consistent volume and controlled intensity as tolerated.
From a practical standpoint, the “logic” users rely on is: if BPC-157 is involved in repair signaling, then pairing it with the right rehab stimulus may help you keep momentum. But the real variable isn’t the peptide name—it’s whether your training load and tissue capacity are moving in the same direction.
Where to be careful
Most claims about BPC-157 are extrapolated from preclinical work or anecdotal reports. In real life, that means you should treat outcomes as uncertain and individualized. I’ve seen athletes interpret short-term improvement as a green light to escalate too fast—then the injury flares. That error has more to do with progression planning than with any supplement or peptide.
What TB-500 is—and why it’s often paired with “migration and repair” narratives
TB-500 is another peptide that’s widely discussed alongside BPC-157. In comparisons, TB-500 is frequently framed around processes like cell migration and tissue remodeling—basically, getting repair activities underway and coordinated.
In my experience, what makes TB-500 discussions confusing is that people sometimes assume it’s a “stronger healing switch.” In practice, the difference between fast gains and slow progress often comes down to: (1) tissue irritability at baseline, (2) how well you manage load, and (3) whether the rehab plan targets the specific tissue and movement pattern that’s failing.
How people typically integrate TB-500 into rehab
- Early rehab consistency: Aim to maintain some functional movement and avoid total deconditioning (within clinician guidance).
- Targeted mechanics: Build strength and control for the exact movement that triggered or worsened the injury.
- Controlled exposure: Progress intensity only when day-to-day symptoms and function remain stable.
If TB-500 is believed to support repair processes, then rehab still provides the mechanical “instruction.” Think of rehab as the language tissue understands; peptides (if they help at all) are the supporting background signal.
Where outcomes can disappoint
Even with a sound plan, not all injuries respond similarly. Partial tears, tendinopathy patterns, joint capsule issues, and nerve-related pain can look similar early but behave differently. If the underlying diagnosis is off, a “peptide protocol” won’t fix the mismatch.
Benefits of BPC-157 and TB-500: what you can realistically measure
When people search for the benefits of bpc 157 and tb500, they often want a clear yes/no on “does it work.” I can’t responsibly give a universal promise, but I can help you measure whether anything is helping using objective markers.
In my workflow, I recommend tracking three buckets over 2–6 weeks (depending on injury severity and rehab design):
1) Function and tolerance
- Pain during specific rehab movements (use the same movement test each time)
- Range of motion at end range (consistently measured)
- Ability to load progressively without symptom spikes
2) Daily symptom pattern
- Morning stiffness duration
- “Pain after activity” next-day response
- Whether symptoms trend down or plateau
3) Training adherence quality
- Did you complete the program consistently?
- Did you advance too quickly?
- Did you reduce rehab when symptoms flared, or push through?
If you don’t improve function while rehab intensity increases appropriately, you’ll likely conclude that the intervention isn’t doing the job for your specific case. That’s not failure—it’s data.
BPC-157 vs TB-500: which one to choose?
The honest answer: it depends on your injury context and your rehab plan. However, here’s a practical decision framework I’ve used when helping people reduce guesswork.
Choose BPC-157-style goals if…
- Your priority is calming local tissue irritability while you rebuild basic capacity
- You’re working on tendon/ligament-type symptoms where you need to tolerate graded loading
- You want a “support” mindset paired with a structured rehab progression
Choose TB-500-style goals if…
- You’re focused on improving repair/remodeling momentum within an overall plan
- Your rehab involves reintroducing movement patterns with consistent technique and progressive exposure
- You’re trying to avoid long plateaus by staying disciplined with mechanics and dosing-adherence routines (within your clinician’s guidance)
But don’t overfit: If your rehab progression is poor, your diagnosis is wrong, or you’re escalating load before the tissue is ready, the “which peptide” question won’t matter much.
Safety, quality, and legality considerations (the part people skip)
This category of peptides is often discussed online, but safety and regulatory status vary widely by country, supplier quality, and intended use. In my hands-on experience working with supplement buyers and athletes, I’ve seen that product sourcing and contamination risk can be a bigger real-world factor than the theoretical mechanism.
- Quality controls: Third-party testing and clear documentation matter.
- Medical context: If you have chronic conditions, take medications, or have a complex injury, talk to a qualified clinician.
- Expect variability: People differ in baseline inflammation, nutrition status, sleep, stress, and rehab adherence.
If you want the best chance of a useful outcome, focus on the basics that reliably influence tissue healing: consistent sleep, adequate protein intake, smart load management, and a rehab plan designed for the specific tissue and movement pattern.
FAQ
What are the benefits of BPC-157 and TB-500?
They’re most commonly discussed for supporting tissue repair and recovery processes. The measurable benefits you should look for are improved function, better tolerance to progressive loading, and a downward trend in next-day symptoms when your rehab intensity rises appropriately.
Can I use BPC-157 and TB-500 together?
Some people combine peptides, but the evidence for combination strategies and precise outcomes is limited. If you’re considering combining approaches, the safest route is to involve a qualified medical professional and treat your rehab progression as the primary driver of results.
How long does it take to see results?
For many soft-tissue recovery efforts, meaningful changes in function and tolerance are often evaluated over weeks rather than days. Use objective markers (function tests, next-day symptom response, and progression quality) rather than relying on short-term “feels better” moments.
Conclusion: a better way to decide
In the BPC-157 vs TB-500 comparison, the most trustworthy takeaway is that “benefits” only become real when paired with a structured rehab plan and objective tracking. BPC-157 discussions tend to emphasize local tissue repair support, while TB-500 discussions emphasize repair/remodeling momentum—but in practice, your rehab mechanics, diagnosis accuracy, and progression quality drive the outcome.
Next step: Pick one approach to align with your current injury stage, then run a 2–4 week measurement plan using consistent functional tests and symptom tracking—so you’ll know whether it’s actually helping you.
Discussion