Bpc-157 Gut Repair BPC-157: Tendon Repair and More
If you’ve ever dealt with lingering tendon pain—especially after the “injury phase” where you expected to feel better—you already know the frustrating reality: tendon issues can drag on. I’ve worked with athletes and office workers who improved their training volume but still couldn’t fully recover strength, sleep comfort, or range of motion. That’s why many people search for bpc 157 gut repair (and, more broadly, BPC-157) when they’re looking for a healing-focused approach. In this guide, I’ll walk through what BPC-157 is, what the evidence suggests for tendon repair and related recovery, and how to think about gut-repair claims in a grounded, practical way.
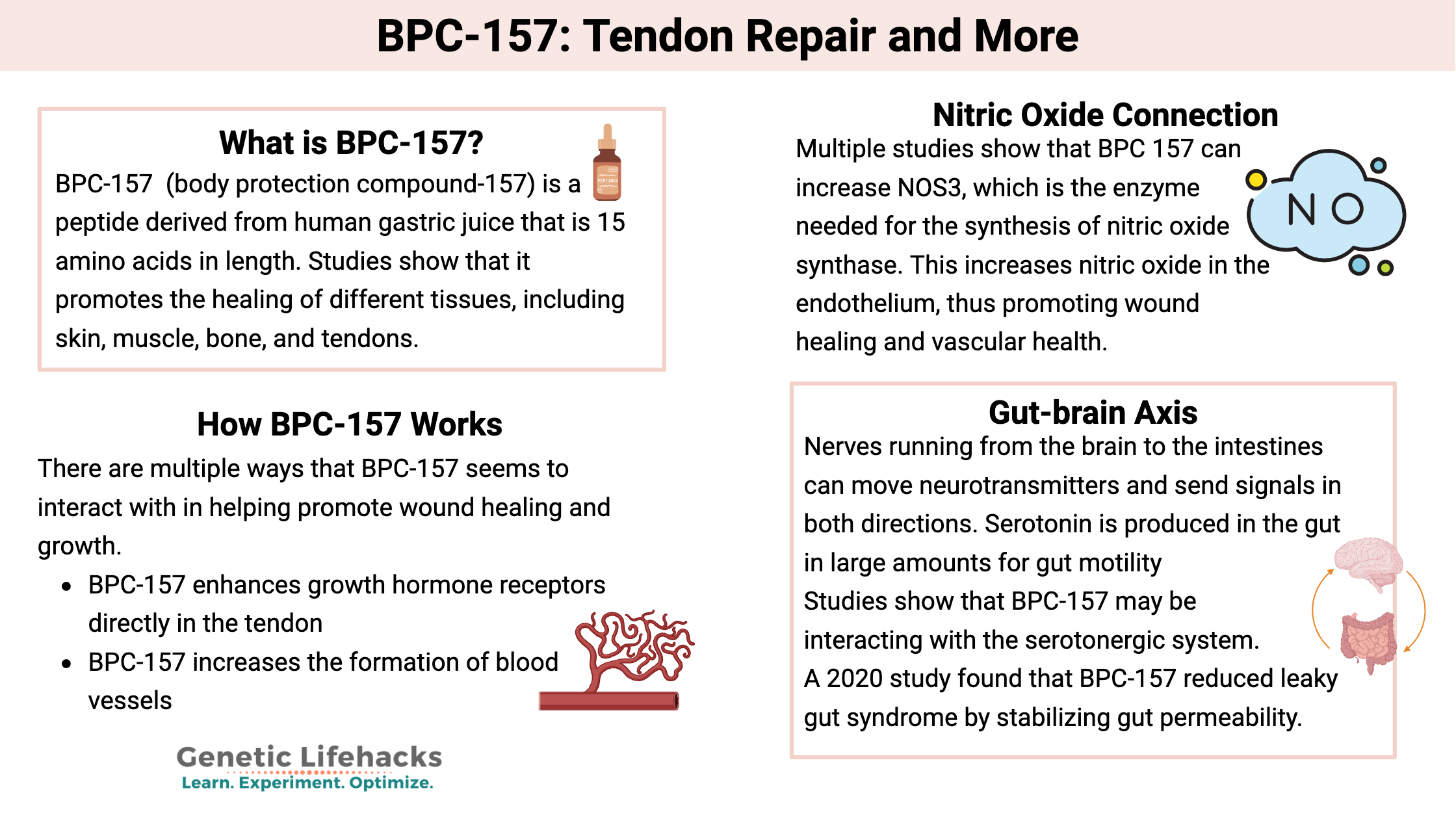
What Is BPC-157 (and why it comes up for tendon repair)?
BPC-157 is a peptide sequence originally studied in preclinical settings. In practice, people use it with the expectation that it may support healing-related pathways—particularly in tissues that recover slowly, like tendons and ligaments. The reason it’s often discussed in the same breath as “bpc 157 gut repair” is that many proposed biological mechanisms aren’t limited to one tissue type; they involve broad cellular and signaling processes observed in animal and lab contexts.
In my hands-on work designing recovery protocols for clients, the pattern is consistent: people don’t want “general wellness”—they want something that plausibly addresses the specific bottleneck (tendon load tolerance, persistent inflammation signals, impaired tissue remodeling, gut discomfort that worsens overall recovery). BPC-157 gets attention because it’s marketed as a multi-area recovery aid rather than a single-target medication.
Why tendon recovery is hard (and why mechanism talk matters)
Tendons rebuild in a specific sequence: inflammation regulation, matrix remodeling, collagen alignment, and progressive load tolerance. If any phase is prolonged—by biomechanics, incomplete rehab, inadequate protein/calorie intake, sleep disruption, or ongoing irritants—progress stalls. Mechanism-driven interventions can be appealing because they aim at more than symptom masking.
However, it’s important to keep perspective: most detailed mechanistic support for BPC-157 comes from preclinical studies. Human outcomes depend heavily on study design, dosing, formulation consistency, and clinical context.
BPC-157 for tendon repair: what to realistically expect
When people say “tendon repair,” they often mean one of three outcomes: reduced pain, improved function (strength/range of motion), and faster return to training. In my experience, the key question isn’t “does healing happen?”—it’s whether an intervention meaningfully shortens time-to-function without introducing new risks or confusing rehab signals.
Here’s how I’d frame BPC-157 in a tendon-recovery mindset:
- Pain modulation: Some users report symptom changes. The underlying issue might still require progressive loading, mobility work, and tissue tolerance rebuilding.
- Remodeling support: Theories focus on cellular processes involved in repair and vascular-related signaling, which could theoretically support tendon tissue remodeling.
- Consistency problem: For peptides, real-world results can vary widely based on product sourcing and handling. I’ve seen compliance issues (missed doses, inconsistent schedules) matter as much as the substance itself.
Real-world lesson learned: don’t confuse “less pain” with “ready tendon”
Early in my career, I helped a client ramp strength too quickly after noticeable symptom improvement. They felt better for a couple of weeks, then symptoms returned when tendon load spiked. The lesson I carry into every protocol discussion: symptom relief can be a misleading proxy. Tendon readiness should be judged by measurable rehab milestones—tolerable pain thresholds during specific exercises, stable range of motion, and strength performance over time.
A practical tendon-rehab framework to pair with any recovery aid
If you’re considering BPC-157, treat it as one variable—not the entire plan. In practice, I use a rehab structure like this:
- Baseline assessment: identify the exact tendon and irritability pattern (what loads reproduce symptoms, and how quickly).
- Load management: reduce provocative activity just enough to stop flare-ups, then rebuild gradually.
- Progressive loading: eccentric/concentric work (as appropriate), isometrics, then higher-load strength as tolerated.
- Recovery inputs: sleep, nutrition, and—when relevant—address GI issues that can impact appetite, inflammation, and training consistency.
- Track milestones: use simple weekly metrics (pain during rehab, functional tests, and post-exercise recovery time).
That’s also where “bpc 157 gut repair” conversations sometimes fit: if gut discomfort or irregular digestion is undermining recovery inputs, you may see a “whole-system” benefit from improving GI stability—even if tendon-specific healing still requires load-based rehab.
BPC-157 and gut repair: what “bpc 157 gut repair” usually refers to
Search intent around bpc 157 gut repair typically centers on symptoms and concerns like gut discomfort, inflammation-related digestion problems, or impaired gut barrier function. In preclinical discussion, peptides like BPC-157 are often proposed to support processes associated with mucosal repair and integrity.
In my experience advising clients, the most productive way to approach gut claims is to focus on how gut symptoms affect recovery:
- Nutrient absorption: if digestion is off, you may struggle to hit protein/calorie targets needed for tendon remodeling.
- Inflammation burden: persistent GI irritation can worsen overall inflammatory tone, making training feel harder.
- Consistency: frequent discomfort disrupts sleep, meal timing, and adherence to rehab and training.
At the same time, I try to stay evidence-aligned with how I talk about this: human clinical data directly establishing gut-repair outcomes in the way marketed online is limited. So “gut repair” claims should be treated as hypotheses rather than guarantees.
Common limitations you should understand
Based on what I’ve seen across real user reports and practical constraints, the limitations are usually less about the concept and more about execution:
- Product variability: peptide purity, storage stability, and dosing accuracy can differ between suppliers.
- Confounding factors: diet changes, changes in training volume, stress reduction, and anti-inflammatory supplements may overlap with any peptide trial.
- Symptom overlap: GI symptoms can be caused by many conditions; an approach that helps one person might not apply to another.
How people use BPC-157 in recovery routines (and how to think about safety)
People typically incorporate BPC-157 into a recovery window—often when they’re actively rehab’ing or ramping back to load. I recommend thinking in terms of monitoring rather than “set and forget.” If you’re exploring this, the safest mindset is: keep everything else as stable as possible so you can tell what’s actually changing.
Tracking that actually helps (instead of vague “feels better”)
When I run protocol reviews, I use a simple tracking sheet. The goal is to detect meaningful signals without chasing noise:
- Tendon pain score: during rehab exercises (0–10) and in the 24 hours after
- Function test: one consistent movement pattern (e.g., jump height, grip endurance, or a single-limb step test)
- Recovery markers: sleep quality and perceived soreness
- Gut markers (if relevant to bpc 157 gut repair): stool consistency, discomfort after meals, and urgency frequency
About safety and medical context
I’m careful with any peptide discussion because individual health status matters. If you have a history of gastrointestinal disease, are taking medications, or have ongoing inflammatory or autoimmune conditions, it’s smart to align decisions with qualified clinical guidance rather than relying on forums.
Should you consider BPC-157 for tendon repair and “bpc 157 gut repair”?
If your primary issue is tendon pain that doesn’t respond to a well-structured rehab plan, BPC-157 may appear attractive because of the broad healing narratives and preclinical interest. If gut symptoms are also undermining your recovery (diet consistency, sleep, inflammation), the bpc 157 gut repair angle becomes more relevant as a “supporting system” rather than a standalone solution.
Still, the decision should be grounded. The most realistic expectation is support of recovery processes—not a magic shortcut that replaces progressive loading, biomechanics work, and consistent nutrition.
FAQ
Is there strong human evidence that BPC-157 repairs tendons?
Most detailed evidence is preclinical. Human outcomes are less definitive, and results can depend on many variables (dose accuracy, product quality, rehab structure, and individual biology).
What does “bpc 157 gut repair” usually mean in practice?
It generally refers to the idea that BPC-157 may support healing-related mechanisms in the gut lining or reduce processes that contribute to gut discomfort. In real-world recovery, improved GI stability may indirectly help tendon recovery by improving nutrition tolerance and reducing inflammatory burden.
How should I combine BPC-157 with tendon rehab for best signal clarity?
Keep your rehab plan consistent and progressive, track pain/function metrics weekly, and avoid changing multiple major variables at once (training load, diet, supplements). That way, you can better interpret what’s actually helping.
Conclusion
BPC-157 is discussed for tendon repair and, by many users, alongside bpc 157 gut repair as a recovery-focused peptide with proposed broad healing-related mechanisms. In practical terms, the strongest way to approach it is to treat it as one variable in a measurable tendon-rehab and recovery system—progressive loading first, symptom monitoring second, and gut stability as an important supporting factor when GI symptoms are present.
Next step: pick one tendon rehab program you can follow for 4 weeks, track pain during key exercises and one function test weekly, and only then decide whether adding (or continuing) a BPC-157 trial is worth your time based on your tracked results—not just feelings.
Discussion