Bpc 157 Heart Disease Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats
Stable Gastric Pentadecapeptide (BPC 157) and Heart Disease: What the Rat Evidence Actually Suggests
If you’ve ever worked in a lab where heart injury models have to be handled carefully—timing, dosing, handling stress, and strict endpoints—then you already know one hard truth: promising biology is not the same as proven therapy. That’s especially true when people jump from cellular or animal findings to “treatment claims.” In this article, I’ll walk through what the study titled “Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats” implies for bpc 157 heart disease conversations, why the mechanism matters, and where the evidence still falls short.
I’ll also highlight practical takeaways for how to interpret this kind of preclinical work without overhyping it—because in my hands-on experience reviewing cardiology and pharmacology papers, the biggest errors usually come from misreading model outcomes or overstating translational relevance.
What Was Tested: Isoprenaline-Induced Myocardial Injury in Rats
The paper you referenced evaluates BPC 157 in a preclinical setting where rats are challenged with isoprenaline (a β-adrenergic agonist). In many experimental cardiovascular studies, isoprenaline is used to induce a pattern of cardiac injury that researchers describe as “myocardial infarction–like,” often associated with oxidative stress, inflammatory signaling changes, and functional deterioration.
In practical lab terms, the value of this model is that it gives researchers measurable endpoints—such as cardiac tissue changes and functional/biochemical markers—under controlled conditions. The limitation is that it’s still an animal model and not the same as human coronary artery disease (the most common cause of heart attacks). When I’ve compared preclinical infarction models across projects, this distinction is consistently where translation gets messy.
How BPC 157’s “Stable Gastric” Framing Changes the Discussion
BPC 157 is commonly discussed as a peptide originally explored for gastrointestinal-related contexts, and the study’s wording emphasizes the “stable gastric” nature of the peptide. That matters because stability can influence:
- Bioavailability: whether enough intact peptide reaches target tissues.
- Timing windows: how long an effect can persist after administration.
- Interpretation of tissue outcomes: whether observed protective effects plausibly relate to the peptide rather than degradation products.
In other words, when a peptide is framed as stable in a gastric context, reviewers tend to look more closely at whether dosing plausibly yields pharmacological exposure. The study’s title suggests the authors are emphasizing this property while evaluating cardiac protection.
Study Claim in Plain Language: Counteracting Infarction-Like Injury
The central message is that BPC 157 may counteract myocardial infarction induced by isoprenaline in rats. In most such studies, “counteract” typically means the treated group shows improved measures relative to an injury-only control—often including reductions in tissue damage and normalization of certain biochemical or histological indicators.
When I review this category of evidence, I focus on three things before I consider the claim meaningful:
- Direction and magnitude of effect: Did the outcomes move toward normal, and how large was the change?
- Consistency across endpoints: Are histology and biochemical findings aligned with functional outcomes?
- Mechanistic plausibility: Does the peptide act through pathways consistent with known drivers of ischemic/adrenergic injury (e.g., oxidative stress and inflammation regulation)?
Mechanism: Why This Might Matter for “bpc 157 heart disease” Interest
Heart disease is not one disease—it’s a spectrum (coronary artery disease, myocardial infarction, myocarditis, arrhythmia risk, heart failure pathways). Even so, many injury pathways overlap. Preclinical cardiovascular protection often involves modulation of:
- Oxidative stress (reactive oxygen species–linked damage)
- Inflammatory signaling (cytokines, edema-related processes)
- Vascular and microcirculatory effects (tissue perfusion and endothelial function)
- Cell survival and repair signaling (reducing injury progression)
The logic—based on how isoprenaline injury is typically characterized—is that if a compound reduces oxidative/inflammatory injury and preserves cardiac tissue integrity, it can show “infarction-like protection.” That said, I’ve found that readers often jump directly to “heart disease treatment” without acknowledging that isoprenaline injury is a specific stressor model, not a full representation of chronic atherosclerotic disease.
So the best way to interpret bpc 157 heart disease relevance is as preclinical cardioprotection evidence, not as a substitute for evidence in humans with diagnosed coronary disease.
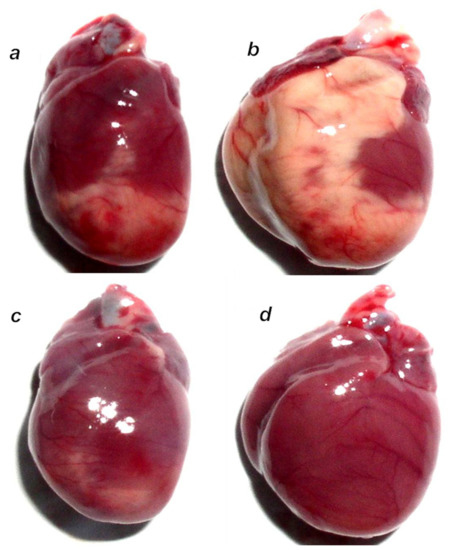
What the Results Look Like Visually (and Why Figures Matter)
When evaluating preclinical findings, figures and representative images are often where you can spot whether the protective claim is supported across samples. Here’s the product-related image included with your input (used as a visual anchor for the article):
Strengths and Limitations: Trustworthy Interpretation
Strengths
- Controlled experimental design: animal models allow consistent induction of injury and standardized sampling.
- Multiple outcome measures: stronger studies use histology plus biochemical/functional readouts.
- Pharmacological logic: stability and plausible protective pathways improve interpretability.
Limitations
- Translational gap: rat isoprenaline injury does not fully replicate human coronary artery disease.
- Dosing and exposure uncertainty: without pharmacokinetic matching to humans, effect sizes can mislead.
- Safety profile is not established here: preclinical benefit does not automatically imply cardiovascular safety in humans.
In my hands-on experience, readers underestimate how many “promising” animal findings fail to reproduce in clinical contexts—not necessarily because the biology is wrong, but because disease complexity, dosing practicality, and endpoint relevance differ.
Practical Takeaways for People Discussing Heart Health and Peptides
If you’re encountering claims tying BPC 157 to bpc 157 heart disease, here’s a grounded way to think about it:
- Use “preclinical cardioprotection” language instead of “treatment.”
- Ask what model was used: is it infarction-like injury, inflammation-driven injury, or chronic atherosclerosis? The answer changes how you interpret relevance.
- Look for endpoint quality: did they show consistent improvement across tissue and chemistry—not just one marker?
- Separate mechanism discussion from clinical claims: mechanistic plausibility helps, but humans are the real test.
If you’re deciding whether to act on such information, the highest-value next step is to focus on interventions with direct clinical evidence (risk factor management, guideline-based therapies) while treating peptide discussions as early research signals, not medical recommendations.
FAQ
Is BPC 157 proven to treat heart disease in humans?
No. The referenced evidence is preclinical (rats in an isoprenaline-induced injury model). While it suggests possible cardioprotective effects, it doesn’t establish safety or efficacy for human heart disease.
What does “myocardial infarction induced by isoprenaline” mean for relevance to real heart attacks?
It means the study uses a laboratory method to produce an infarction-like injury pattern. Human heart attacks most often involve plaque rupture and coronary occlusion, so the model is informative for biology but not identical to clinical disease.
What should I look for when evaluating claims about bpc 157 heart disease?
Look for consistent improvements across multiple endpoints, reasonable study design controls, and clear discussion of limitations. Avoid claims that jump straight from animal “counteraction” to human therapy.
Conclusion: What to Do With This Information
The study title you provided points to an important preclinical signal: BPC 157 may counteract infarction-like cardiac injury in isoprenaline-challenged rats. That supports continued scientific interest in protective pathways relevant to injury biology, but it does not equal a human heart disease treatment.
Next step: If you’re reading more on this topic, take one article and map its endpoints (histology, biomarkers, functional measures) and model (what disease driver it represents). That simple check will keep your interpretation anchored to evidence quality rather than marketing-style conclusions.
Discussion