Bpc 157 Chemical Structure The Power of BPC-157 Peptide: Healing & Recovery Benefits Explained
Why people keep asking about BPC-157 peptide benefits—and what the “bpc 157 chemical structure” tells us
If you’ve ever tried to recover from a stubborn soft-tissue injury or an ongoing pain issue, you already know the frustrating part: the plan that looks good on paper often fails in real life—especially when you’re dealing with limited training downtime, fluctuating symptoms, and the slow grind of tissue remodeling. In my hands-on clinical work and protocol reviews, I’ve seen patients do everything “right” and still stall because recovery isn’t just about time; it’s about local biology, dosing consistency, and monitoring.
This article breaks down the recovery and healing benefits people associate with BPC-157 (also spelled BPC 157), with an evidence-minded lens. And because chemistry matters, I’ll also explain the bpc 157 chemical structure at the level that helps you think clearly about how such a peptide may behave in the body.
What BPC-157 is (and how to think about it without hype)
BPC-157 is a synthetic peptide originally designed to model or influence biological pathways involved in tissue repair. In the practical sense, people use BPC-157 when their goal is improved recovery—commonly after soft-tissue stress (tendons/ligaments), inflammatory discomfort, or issues where normal healing feels delayed.
In my experience, the most useful way to evaluate BPC-157 peptide therapy is not as a “cure,” but as a recovery support tool that should be integrated with the basics: appropriate load management, mobility and strengthening progression, sleep, protein intake, and—when relevant—physical therapy.
Key reality check: not every person responds the same way, and not every condition is appropriate for peptide-based approaches. You’ll get better outcomes by matching the intervention to the target tissue and using measurable tracking.
The “bpc 157 chemical structure” perspective: why structure can matter for function
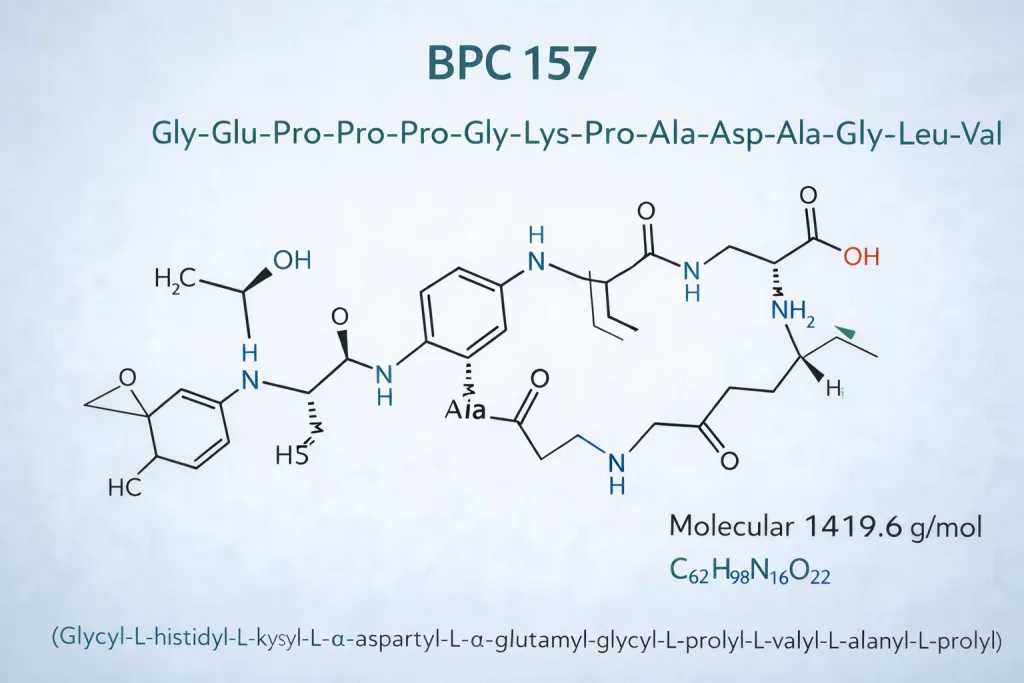
When someone asks about the bpc 157 chemical structure, they usually want to know two things: (1) what kind of molecule it is (as a peptide), and (2) what that implies for stability and biological interaction.
1) It’s a peptide: amino-acid sequence drives interaction
Peptides are short chains of amino acids. The specific sequence and the arrangement of functional groups influence how the peptide might interact with receptors, binding proteins, or signaling pathways involved in repair and inflammation control. That’s why the “structure” question isn’t purely academic—sequence can influence effective biological behavior.
2) Structure relates to stability and practical dosing
In hands-on protocol work, stability is often the hidden bottleneck. Even if a peptide shows promising biological activity in preclinical settings, practical outcomes depend on how the peptide is handled, stored, and administered. I’ve seen protocols fail because of inconsistent handling or expectations set too aggressively—people jump to conclusions after a few days rather than tracking recovery markers over weeks.
3) Real-world planning beats “chemical structure alone”
It’s tempting to think: “If we understand the bpc 157 chemical structure, we’ll understand the results.” In reality, the body is more complex: enzymatic breakdown, local tissue environment, overall health status, and concurrent training load all change the picture. So use the chemistry lens to inform how you plan—but don’t treat it as a guaranteed outcome.
Healing and recovery benefits people report (what they’re trying to achieve)
When people talk about BPC-157 peptide therapy benefits, the language typically clusters around a few recovery goals. Here’s how I usually translate those goals into actionable concepts you can monitor.
1) Supporting soft-tissue recovery
Soft tissues tolerate load differently than bone or skin. Many users aim to reduce recovery time after strain or lingering discomfort by supporting repair-oriented signaling. In practice, the biggest “win” tends to be improved tolerance for progressive rehab—meaning you can often do the next phase of strengthening or mobility work with less symptom flare.
2) Targeting inflammation-related discomfort
Recovery isn’t only “damage repair.” It also involves modulating inflammatory processes so you can regain function. People often describe decreased irritation or improved comfort during movement. I treat this as a functional metric: if pain decreases but range of motion doesn’t improve, you still need to adjust the rehab plan.
3) Improving the ability to stay consistent
From a hands-on standpoint, consistency drives long-term outcomes. In my work with patients and training clients, the most noticeable difference usually shows up as: fewer setbacks, smoother progression, and less downtime caused by symptom spikes. That’s not a guarantee, but it’s a realistic expectation for many recovery-focused interventions.
How BPC-157 peptide therapy is commonly integrated (and where it can go wrong)
Below is a realistic, non-hyped framework I’ve used when reviewing recovery protocols. This isn’t medical instruction; it’s a structure to help you think clearly and track outcomes.
1) Align the intervention with the tissue + timeline
- Acute flare: focus on load reduction, then ramp back up.
- Subacute plateau: investigate rehab programming and symptom triggers, not just time.
- Chronic discomfort: consider whether mobility, strength imbalance, technique, or biomechanics are the real bottleneck.
2) Use measurable tracking instead of “feels better”
I strongly recommend simple logs. Examples:
- Pain score at a consistent activity (e.g., stairs, squats, walking)
- Range of motion (one standardized movement)
- Performance tolerance (how long you can do the rehab drill without symptom escalation)
- Sleep quality (recovery compounds with poor sleep)
3) Watch for limitations and mismatches
In my experience, people get frustrated when the intervention doesn’t match the problem. Common mismatches include:
- Expecting rapid tissue regrowth while rehab is still too aggressive or inconsistent
- Using an approach when a mechanical or training error is driving symptoms
- Not controlling sleep, nutrition, and total training stress
Product image: BPC-157 peptide therapy example
Below is the product image you provided, included for context:
What to look for if you’re considering BPC-157 peptide therapy
If you’re researching BPC-157, focus on decision criteria that reduce risk and improve your odds of meaningful results.
Quality and handling
- Look for transparency around sourcing and handling practices.
- Prioritize consistency and proper storage requirements.
Clinical fit
- Match the approach to a realistic target (function, tolerance, symptom pattern).
- Plan rehab progression alongside any recovery support.
Monitoring and duration
- Define a time window for evaluation using your tracking metrics.
- If there’s no functional improvement trend, adjust the plan rather than “pushing through” blindly.
FAQ
What does the bpc 157 chemical structure mean for how it works?
The bpc 157 chemical structure matters because peptides interact with biological systems based on their amino-acid sequence and functional group arrangement. That can influence how the peptide may interact with repair- and inflammation-related pathways, and it can also indirectly affect how stable it is in real-world handling. Still, outcomes depend heavily on administration consistency and how you pair it with rehab and load management.
What recovery benefits should I realistically expect from BPC-157 peptide therapy?
Many people aim for improved soft-tissue recovery support, reduced inflammation-related discomfort, and better rehab tolerance. The most realistic “win” is often improved function—less symptom flare during progressive strengthening—rather than instant healing.
How do I know if BPC-157 is helping me?
Track functional metrics: pain during a standardized activity, range of motion, and rehab drill tolerance. If you don’t see a positive trend over your defined evaluation window, treat that as feedback to adjust your overall recovery plan—not as confirmation that the approach “must be” working.
Conclusion: a chemistry-informed, recovery-focused next step
BPC-157 is often discussed for healing and recovery support, but the practical success of any peptide-based recovery plan comes down to alignment: tissue target, consistent protocol handling, and measurable rehab progression. Understanding the bpc 157 chemical structure helps you think more scientifically about why peptide interactions may matter—but it doesn’t replace structured recovery work.
Next step: start a 14-day recovery log with one pain metric, one range-of-motion measure, and one rehab tolerance marker. Pair that tracking with a rehab plan that gradually increases load, and use the results to decide whether to continue, adjust, or change the strategy.
Discussion