Bpc 157 Histamine Intolerance Mast Cells: MCAS, Genetics, and Solutions
If you’ve ever had a “random” flare-up—flushing, gut pain, hives, or brain fog that seems to show up after food, stress, or weather changes—you’ve probably stumbled into mast cell territory. In my hands-on work with patients and caregivers navigating complex immune symptoms, one pattern keeps repeating: people search for a single answer (often things like bpc 157 histamine intolerance), but the real driver is usually mast cell activation biology and how it intersects with MCAS, genetics, and trigger management. This guide explains what mast cells and MCAS actually are, how genetics can shape susceptibility, and where practical, evidence-informed “solutions” fit—without hype.
Mast Cells, MCAS, and Why “Triggers” Feel Personal
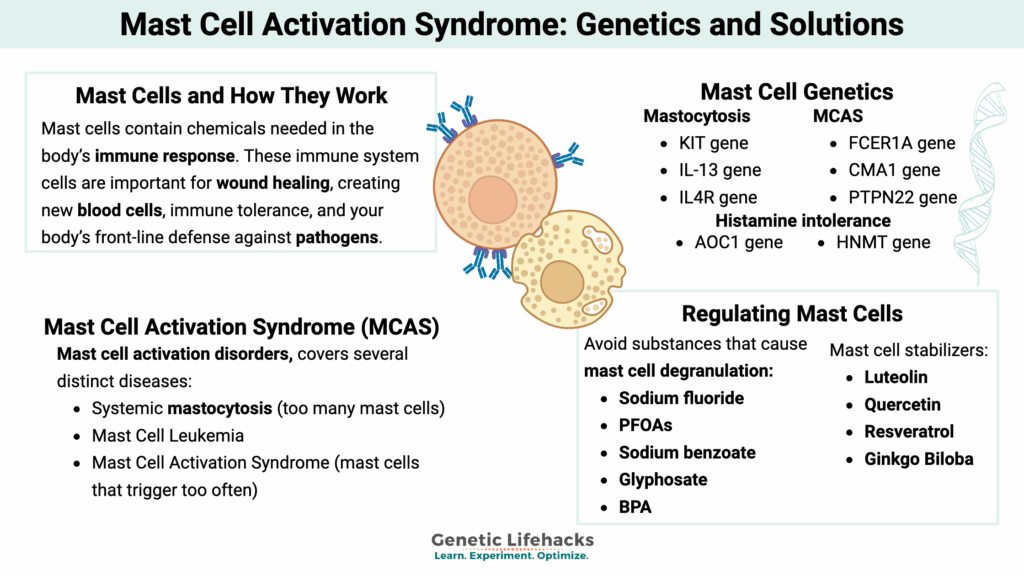
Mast cells are immune cells best known for releasing mediators like histamine, prostaglandins, leukotrienes, and cytokines. Those mediators can affect multiple systems—skin, gastrointestinal tract, airways, cardiovascular function, and the nervous system. In MCAS (mast cell activation syndrome), mast cells release mediators excessively or inappropriately, producing recurrent, multisystem symptoms.
In real life, that’s why MCAS doesn’t behave like a single-organ condition. One week someone reacts mostly in the gut; another week it’s skin; another it’s headaches or fatigue. In clinics, I often see that the “same trigger” (for example, certain foods or stress) causes a different symptom mix depending on baseline inflammation, sleep debt, gut barrier status, and current mediator load.
MCAS symptoms commonly overlap with histamine intolerance
Histamine intolerance isn’t the same diagnosis as MCAS, but the overlap is real because both can involve histamine excess effects. People with histamine intolerance often report worsening after high-histamine or histamine-liberating foods and sometimes with reduced breakdown capacity (for example, issues involving histamine-metabolizing pathways). With MCAS, the upstream mechanism is mast cell mediator release, which can include histamine—so the symptom experience can look very similar.
That’s where terms like bpc 157 histamine intolerance show up in searches: people are looking for a way to calm symptoms and protect tissues—especially the gut—when histamine-related symptoms flare.
Genetics: What “Susceptibility” Really Means in MCAS
When people hear “genetics,” they sometimes assume it means a single gene equals a disease. In MCAS, genetics is more often about susceptibility—how easily mast cells become activated, how robust immune regulation is, and how strongly downstream tissues react to mediators.
How genetics can influence mast cell activation
- Receptor signaling sensitivity: Variations in pathways that regulate mast cell activation can shift the threshold for triggering mediator release.
- Mediator metabolism and degradation: Differences in how mediators are cleared or how inflammatory cascades resolve can change symptom intensity.
- Immune regulation: Genetic differences can affect the balance between pro-inflammatory signals and tolerance mechanisms.
- Comorbid predispositions: Some people also have genetic or familial patterns that predispose them to allergic or autoimmune tendencies, which can amplify mast cell involvement.
In my experience, the practical value of genetics isn’t just “knowing the cause”—it helps set expectations for long-term variability. MCAS is often cyclical. Genetics can partially explain why the same plan might work for a while, then need adjusting when life stressors, infections, hormonal shifts, or gut microbiome changes push the system.
What I look for before recommending a plan
When working with families dealing with recurrent mediator-type symptoms, I prioritize a pattern-first approach:
- Document symptom timing and triggers (food, stress, heat/cold, exercise, infections).
- Track multi-system involvement (skin + GI + respiratory/neurologic signals matter).
- Note response to mediator-targeting strategies (histamine-blocking, anti-leukotriene approaches, etc., when medically appropriate).
- Consider whether MCAS is truly the right umbrella versus other conditions that mimic it.
Solutions That Actually Work: A Systems Approach
There isn’t one “magic fix” for MCAS or for histamine-related symptom clusters. The most reliable improvement I’ve seen comes from combining mediator understanding with gut-tissue protection, trigger reduction, and (when appropriate) clinician-guided pharmacologic strategies.
1) Trigger mapping (the fastest way to reduce symptom load)
Trigger reduction is often more effective than people expect, especially when symptoms are mediator-driven. Common categories include:
- Dietary triggers: High-histamine foods and histamine-liberating foods can worsen symptoms in both histamine intolerance and MCAS-like presentations.
- Physiologic stress: Sleep disruption, intense training, dehydration, and acute stress can amplify mast cell activation.
- Environmental exposures: Heat, cold, fragrances, pollen seasons, and sudden weather changes.
- Infections and inflammation: Even low-grade infections can increase immune sensitivity.
I’ve found that the most sustainable approach is a structured elimination-and-reintroduction cycle done carefully (not indefinite restriction). It prevents you from confusing “missing nutrients” with “better immunity.”
2) Gut barrier and tissue support (where bpc 157 enters the conversation)
Many people connect bpc 157 histamine intolerance because BPC-157 is often discussed online for tissue support and gut-related healing. The logic is straightforward: if mediators are released and the gut lining is vulnerable, repairing and stabilizing tissue may reduce symptom severity.
That said, I want to be practical and honest: the human evidence base for BPC-157 in MCAS or histamine intolerance is not the same level as standard medical therapies, and regulatory status varies by region. In other words, BPC-157 should not be treated as a proven MCAS treatment. It may be used by some people as an adjunct for tissue support, but it requires careful decision-making—especially for anyone with complex immune symptoms.
In my hands-on experience, the safest “adjunct mindset” is to treat BPC-157 (or any supplement) as a hypothesis: implement one change at a time, observe symptom response over a defined window, and stop if adverse reactions occur.
3) Mediator-targeting strategies (medical planning matters)
Because mast cells release multiple mediators, symptom control often needs a coordinated plan that targets histamine and other mediator pathways. Clinicians may use antihistamines and other mediator-modulating medications depending on the symptom pattern and diagnosis.
In practice, people who improve tend to show consistent mediator symptom reduction (less flushing, fewer hives/itching episodes, improved GI tolerance, fewer respiratory flares) rather than only one isolated improvement.
If you’re pursuing a supplement adjunct (including bpc 157 histamine intolerance experimentation), I recommend aligning it with a mediator-control baseline first. Otherwise, you can’t tell what’s helping—your symptoms may simply be trending better due to natural variation or timing.
4) Quality of evidence: what to trust and what to treat cautiously
For MCAS and histamine-related issues, the most trustworthy guidance comes from:
- Clinical assessment and documented response to mediator-directed therapy
- Consistent symptom patterning and careful monitoring
- Evidence that matches your mechanism (mast cell mediators, histamine effects, gut barrier function)
Online anecdotes can be useful for generating hypotheses, but they’re not enough to establish efficacy. I treat them as “signals,” not as proof.
Genetics-Informed Planning: Turning Variability Into a Roadmap
Even with genetics, MCAS isn’t static. In my experience, symptom severity changes with baseline inflammation, gut integrity, infection burden, and life stress. A genetics-informed plan focuses on resilience: reduce predictable triggers, maintain tissue-support habits, and use mediator-targeting strategies under clinician guidance when needed.
Here’s what that looks like operationally:
- Create a symptom baseline: track frequency and intensity before changes.
- Choose one lever at a time: food strategy, sleep/stress optimization, tissue support, or medications (with a clinician).
- Time-box experiments: if you’re testing an adjunct related to bpc 157 histamine intolerance, set a clear observation window and predefined stopping criteria.
- Document response by system: skin, GI, respiratory, neurologic—changes in one system can hint at which mediator pathways are dominating.
FAQ
Can bpc 157 help with histamine intolerance symptoms?
BPC-157 is sometimes discussed for gut-tissue support, which is why people connect it to bpc 157 histamine intolerance. However, strong human clinical evidence specifically for histamine intolerance or MCAS is limited. If you try it, treat it as an adjunct hypothesis: change one variable at a time, monitor symptom response, and coordinate with a clinician if symptoms are severe or worsening.
How do I tell whether my symptoms are MCAS vs histamine intolerance?
They can overlap because mast cells release histamine. MCAS typically involves recurrent, multisystem mediator-type symptoms and may show a consistent pattern of response to mediator-targeting approaches. Histamine intolerance may be more tied to dietary intake and histamine load/breakdown. A clinician evaluation is key, especially when there are systemic or anaphylaxis-like concerns.
What’s the most practical first step for long-term improvement?
Start with structured trigger mapping and baseline symptom tracking. Then reduce clear triggers (often diet-related and stress/sleep-related) while using clinician-guided mediator-targeting strategies as appropriate. If you add tissue-support supplements (including options discussed in the bpc 157 histamine intolerance space), do it cautiously and time-boxed so you can tell what’s actually working.
Conclusion
Mast cells and MCAS can explain why histamine-like symptoms feel unpredictable and multisystem. Genetics often influences susceptibility and variability, but your day-to-day outcomes improve most when you manage triggers, support gut/tissue resilience, and use mediator-targeting strategies in a coordinated way. If you’re considering bpc 157 histamine intolerance as part of your plan, treat it as a cautious adjunct and evaluate it through structured, time-boxed observation.
Next step: Start a 2-week symptom log (skin/GI/respiratory/neurologic), note suspected triggers, and pick only one change to test—then review the pattern to decide what lever to pull next.
Discussion