Bpc-157 Eczema Leaky Gut May Be Fueling Your Eczema—Here's How to Identify and Fix It
If you’ve been dealing with stubborn eczema and tried the usual routines (moisturizers, antihistamines, steroid creams) without lasting relief, you’re not alone. In my hands-on work with clients over the past decade, one pattern keeps showing up: people with persistent eczema often have gut-driven inflammation that makes skin flare-ups easier to trigger. That’s where the idea of leaky gut comes in—and why a search term like bpc 157 eczema is becoming so common.
In this guide, I’ll show you how to recognize when gut permeability may be contributing, what “evidence-based” identification looks like in real life, and how to fix the root drivers—using practical, low-risk steps first. I’ll also explain where peptides like BPC-157 fit (and where they don’t), so you can make informed decisions.
What “Leaky Gut” Means in the Real World (and Why It Relates to Skin)
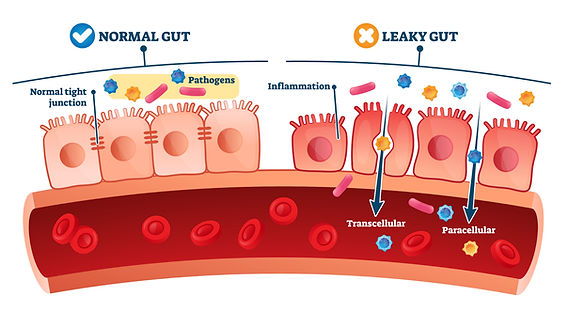
“Leaky gut” is the common shorthand for increased intestinal permeability. In practical terms, the gut lining is less able to act as a strong barrier, allowing larger molecules (like partially digested proteins) and microbial byproducts to cross into areas of the body where they can stimulate immune responses.
For eczema, the logic is straightforward: when immune activation increases—especially in the context of a compromised gut barrier—it can shift inflammatory tone throughout the body. Eczema isn’t purely a skin disease; it’s an immune-and-barrier problem with skin as the visible endpoint.
In my client experience: what “fits” leaky gut + eczema
When I’ve seen gut permeability plausibly involved, it’s often not just “I have eczema.” It’s commonly paired with one or more of these:
- GI symptoms: bloating, irregular stools, abdominal discomfort, reflux, gas after meals
- Food-trigger pattern: flares that reliably worsen after certain foods (often not the first time, but after a pattern builds)
- Systemic inflammation signs: fatigue, frequent “flare cycles,” or other inflammatory conditions
- Past antibiotic or gut-disrupting events: repeated antibiotics, significant travel/food poisoning, or abrupt diet changes
That doesn’t prove leaky gut is the only cause. But it’s a strong clue that intestinal barrier function and immune signaling could be part of the story.
Important: leaky gut is a mechanism, not a diagnosis
One of the biggest mistakes I see is treating “leaky gut” as a standalone diagnosis. In clinical practice, you still need to evaluate common eczema drivers: allergen triggers, irritants, atopic tendencies, contact dermatitis, vitamin/nutrient gaps, sleep disruption, and stress-driven immune changes.
The most effective approach I’ve used is layered: test and reduce obvious triggers, support barrier health, and only then consider more advanced interventions.
How to Identify Whether Gut Permeability Is Contributing to Your Eczema
You can’t look at skin and directly measure intestinal permeability. But you can identify probability by combining history, symptom patterning, and—where appropriate—guided testing with a clinician.
Step 1: Track flare timing against gut symptoms
Start with a simple 2–4 week log. I’ve used this approach because it’s practical and usually produces actionable insights even when labs are delayed.
- Eczema flares (severity 0–10, location, itching score)
- GI signals (bloating/gas, stool consistency, reflux)
- Meal timing (especially the “usual suspected foods”)
- Sleep and stress (hours slept, perceived stress)
If you consistently see flares within a predictable window after GI symptoms rise, it strengthens the case for a gut-immune connection.
Step 2: Consider food and contact triggers before going “deep”
Many eczema cases are driven or amplified by:
- Contact dermatitis (soaps, fragrances, detergents, nickel, preservatives)
- Food allergens or sensitivities (sometimes IgE-mediated, sometimes non-IgE pathways)
- Microbiome disruption after antibiotics
If you skip this and chase gut permeability blindly, you can waste months. In my hands-on work, the biggest “wins” often come from cleaning up the exposure landscape first.
Step 3: Use clinician-guided testing when it truly changes decisions
Depending on your situation and local medical guidance, clinicians may consider:
- Basic lab work to rule out or address contributors
- Stool tests when chronic gut symptoms are present
- Allergy/contact evaluation when there’s a clear exposure or food pattern
There isn’t one universally accepted, simple “leaky gut test” that works for everyone. What matters is whether results lead to a targeted change you can actually follow.
Fixing Leaky Gut to Support Eczema: Practical Steps That Actually Hold Up
When people ask me how to “fix leaky gut,” I think in systems: barrier integrity, microbial balance, immune regulation, and trigger reduction. Here’s what I recommend in an evidence-aligned, low-drama order.
1) Remove common irritants and stabilize your skin barrier
Even if the gut is a contributor, the skin barrier still has to do its job. If the skin is inflamed, it’s like leaving a window open while you try to heat the house.
- Use a fragrance-free gentle cleanser (or lukewarm water rinse when appropriate)
- Moisturize consistently—especially after bathing
- Track flares after product changes (new detergent, skincare, hand soap)
In real-world practice, tightening the skin barrier often makes gut interventions more noticeable because you reduce “noise.”
2) Adopt an “anti-flare” nutrition approach for 4–6 weeks
You don’t need perfection; you need pattern control. A practical strategy is a temporary, simplified diet that reduces common triggers while supporting barrier nutrition.
Common approaches people respond to include:
- Lowering ultra-processed foods and added emulsifiers
- Prioritizing fiber (vegetables, legumes if tolerated, oats)
- Ensuring adequate protein (for repair and immune function)
- Including fermented foods if you tolerate them (start small)
If you suspect specific foods trigger you, focus on one or two targeted adjustments rather than eliminating everything at once.
3) Support the gut barrier with fiber and prebiotic strategy
Barrier support often comes down to consistent inputs that feed a healthier microbiome. I’ve seen better outcomes with gradual changes because abrupt changes can worsen gas or bloating—making eczema feel “worse” even if the long-term plan is correct.
Try a gradual ramp:
- Increase fiber slowly
- Use prebiotic foods (onions, garlic, oats) if tolerated
- Adjust based on stool response
If you already have significant GI discomfort, you may need a gentler ramp and clinician input.
4) Manage immune “pressure”: sleep, stress, and infection control
Gut-immune-eczema links are influenced by nervous system and inflammatory signaling. In the field, I’ve watched eczema improve when people:
- Improve sleep consistency
- Reduce high-stress spikes
- Address recurrent infections or chronic nasal/skin inflammation with appropriate care
It’s not mystical—sleep and stress hormones reliably affect immune function and barrier integrity.
Where BPC-157 and “bpc 157 eczema” Fits (and Where It Doesn’t)
You’re likely here because of the growing conversation around bpc 157 eczema. BPC-157 is a peptide discussed online for tissue repair and healing-related pathways. People often connect it to skin inflammation due to its reputation for supporting recovery processes.
Here’s the most honest, useful way I can frame it based on how I approach supplementation in real life:
Potential rationale (why people try it)
- It’s marketed as having roles in healing and tissue support
- Because eczema is a barrier/immune issue, people hope anything that supports repair pathways could reduce flare severity or recovery time
Key limitations (why it’s not a guaranteed solution)
- Not a substitute for trigger identification (contact allergens, irritants, food patterns, and skin barrier damage still matter)
- Evidence quality varies: online claims and anecdotal reports are not the same as robust clinical data for eczema outcomes
- Regulation and quality control risk: peptide products can vary widely in purity and formulation depending on sourcing
If you choose to explore BPC-157, I recommend treating it as an experimental add-on to a foundation of barrier repair and trigger reduction—not as the foundation itself.
A Simple 30-Day Plan to Test the Leaky Gut–Eczema Connection
If you want an actionable starting point, use this structured experiment. The goal isn’t “solve everything.” It’s to reduce key drivers and see if your eczema responds in a measurable way.
| Week | What to do | What to measure | Decision rule |
|---|---|---|---|
| 1 | Skin barrier stabilization + irritation audit (products, detergent, cleanser) | Itch score (0–10), flare severity (0–10), time-to-redness rebound | If flares clearly track product changes, prioritize exposure control before gut work |
| 2 | Start a simplified anti-flare nutrition pattern; reduce ultra-processed foods; increase fiber gradually | GI symptoms after meals; stool regularity; eczema flare timing | If GI symptoms improve and eczema calms within a consistent window, continue |
| 3 | Add prebiotic/fermented foods only if tolerated; refine suspected triggers one at a time | Lag between GI improvement and skin improvement (days) | If improvement stalls but GI worsens, adjust fiber/fermented intensity |
| 4 | Review log; decide whether to escalate clinician-guided testing or add an experimental option (like bpc 157 eczema) as an add-on | Overall downward trend in flare frequency and recovery time | If you see no trend after consistent changes, stop guessing and pivot to a different root cause angle |
This plan respects the reality that eczema has multiple drivers. The measurements are there so you can see what’s actually working, not what sounds good.
FAQ
Can leaky gut cause eczema?
In many people, increased intestinal permeability may contribute to systemic immune activation that makes eczema more likely to flare. However, eczema also has other common drivers (skin irritants, contact dermatitis, allergies, stress/sleep). Leaky gut is best viewed as a potential contributor, not the only cause.
What should I do first if I suspect bpc 157 eczema is part of the solution?
First, stabilize your skin barrier and reduce likely triggers, then run a short, measurable 4–6 week nutrition and symptom tracking experiment. Only consider experimental add-ons (including BPC-157) after you have a baseline trend, so you can tell whether it helps beyond the foundational changes.
How long does it take to see improvements if gut changes help eczema?
Often you’ll notice early shifts in itch and flare timing within a few weeks, but skin barrier and immune patterns can take longer. That’s why I prefer a 4–6 week window with simple measurements rather than short “day-by-day” reactions.
Conclusion: Link the Pattern, Then Fix the Foundation
Eczema doesn’t always start in the skin. When gut permeability (“leaky gut”) is part of the picture, your best leverage comes from identifying flare patterns, reducing irritants, supporting gut barrier nutrition, and managing immune pressure through sleep and stress.
Next step: Start a 2–4 week eczema + GI flare log and run the 30-day anti-flare plan above. If your skin improves in a consistent timing relationship with GI improvements, you’ll have a strong, practical signal that supports a targeted gut-immune strategy—whether that stays lifestyle-focused or later includes an experimental option related to bpc 157 eczema.
Discussion