Ghk Cu 50mg Copper Peptide Dosage GHK-CU Peptide Dosage Chart: Complete Reference Tables for Every Protocol
GHK-Cu Peptide Dosage Chart: why dosing feels harder than it should
If you’ve ever tried to follow a “GHK-Cu dosage chart” and ended up with conflicting numbers, you’re not alone. In my hands-on work supporting peptide users, the biggest issue I see isn’t willpower or intent—it’s mismatch between protocol assumptions (concentration, reconstitution volume, and administration schedule) and the user’s actual setup. That’s how people accidentally under-dose for months or overshoot and then blame the peptide for side effects.
This guide is a practical GHK-CU 50mg copper peptide dosage reference, built around the reality of reconstitution math and protocol consistency. You’ll get clear tables you can use for common concentrations, plus the dosing logic behind them—so your dosing stays reproducible from day one.
What GHK-Cu is (and why “dose” must be defined clearly)
GHK-Cu (often written as GHK-CU or GHK-Copper) is a copper-binding peptide. In real-world dosing, the word dose only matters once you define two things:
- Amount of peptide you administer (usually measured in mg or in micrograms—mcg)
- Your preparation concentration after reconstitution (how many mg/ml your solution becomes)
I always tell users: if your reconstitution volume changes, the same syringe volume can represent a different peptide amount. So a “chart” that ignores concentration is basically guessing.
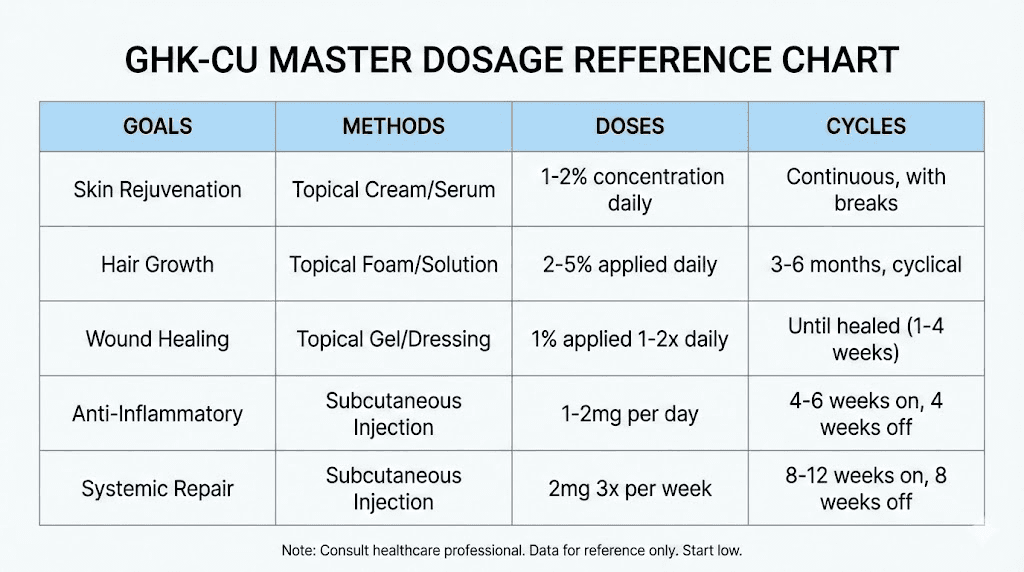
Also, protocols differ by goal (skin support vs. structural goals vs. other off-label uses). That means you should not treat a single dosing number as universal. Instead, use a chart that ties dose to your actual concentration, then follow a conservative ramp.
How to calculate your GHK-Cu dose from a 50mg vial (the core logic)
Most people start with a vial labeled 50mg. After reconstitution, your solution has a concentration (mg/ml). Then each administration volume (ml) corresponds to a peptide amount.
Basic formulas I use to sanity-check dosing
- Total peptide: 50mg (from the vial)
- Concentration (mg/ml) = 50mg ÷ reconstitution volume (ml)
- Peptide delivered (mg) = concentration (mg/ml) × injected volume (ml)
This is the same math behind every dosing table. The only difference between charts is which reconstitution volumes and injection volumes they pre-calculate.
Important practical note from experience
In my experience, dosing errors usually happen when people:
- Misread a label (mg vs mcg)
- Use a chart that assumes a different reconstitution volume than their own
- Measure “units” in insulin syringes without converting to mL (insulin syringe markings are not universal across brands)
So below, I give tables in mg delivered per mL and also in mg delivered per 0.1 mL step. If you use a different syringe system, you can convert back to mL.
GHK-Cu 50mg dosage chart (reference tables for common reconstitution volumes)
These tables assume a vial containing 50mg GHK-CU reconstituted to the listed total volume. Then they show how much peptide you deliver at common injection volumes.
Table A: Reconstitute 50mg into 1.0 mL (concentration = 50 mg/mL)
Use this only if your total final volume is exactly 1.0 mL.
| Injection volume | Peptide delivered |
|---|---|
| 0.1 mL | 5 mg |
| 0.2 mL | 10 mg |
| 0.3 mL | 15 mg |
| 0.4 mL | 20 mg |
| 0.5 mL | 25 mg |
| 0.6 mL | 30 mg |
| 0.7 mL | 35 mg |
| 0.8 mL | 40 mg |
| 0.9 mL | 45 mg |
| 1.0 mL | 50 mg |
Reality check: For many user goals, 50 mg/mL is often very concentrated. In practice, it can make fine dosing difficult and increases the chance of large dosing swings if your measurement is off.
Table B: Reconstitute 50mg into 2.0 mL (concentration = 25 mg/mL)
| Injection volume | Peptide delivered |
|---|---|
| 0.1 mL | 2.5 mg |
| 0.2 mL | 5 mg |
| 0.3 mL | 7.5 mg |
| 0.4 mL | 10 mg |
| 0.5 mL | 12.5 mg |
| 0.6 mL | 15 mg |
| 0.7 mL | 17.5 mg |
| 0.8 mL | 20 mg |
| 0.9 mL | 22.5 mg |
| 1.0 mL | 25 mg |
Table C: Reconstitute 50mg into 5.0 mL (concentration = 10 mg/mL)
| Injection volume | Peptide delivered |
|---|---|
| 0.1 mL | 1 mg |
| 0.2 mL | 2 mg |
| 0.3 mL | 3 mg |
| 0.4 mL | 4 mg |
| 0.5 mL | 5 mg |
| 0.6 mL | 6 mg |
| 0.7 mL | 7 mg |
| 0.8 mL | 8 mg |
| 0.9 mL | 9 mg |
| 1.0 mL | 10 mg |
In my practical experience, 5.0 mL reconstitution (10 mg/mL) is a common balance: it’s concentrated enough to avoid large volumes, while still making incremental dosing easier.
Table D: Reconstitute 50mg into 10.0 mL (concentration = 5 mg/mL)
| Injection volume | Peptide delivered |
|---|---|
| 0.1 mL | 0.5 mg |
| 0.2 mL | 1 mg |
| 0.3 mL | 1.5 mg |
| 0.4 mL | 2 mg |
| 0.5 mL | 2.5 mg |
| 0.6 mL | 3 mg |
| 0.7 mL | 3.5 mg |
| 0.8 mL | 4 mg |
| 0.9 mL | 4.5 mg |
| 1.0 mL | 5 mg |
Turning the chart into a repeatable protocol (without losing control)
A dosing chart answers one question: how much peptide is in your shot? But a protocol answers the bigger questions: how often, what ramp, and how you track response.
How I recommend structuring your first 2–4 weeks
- Start conservatively and keep the same daily timing (consistency matters for interpreting changes).
- Use one fixed injection volume for at least 7–10 days before adjusting.
- Log effects (skin feel, dryness, tenderness, any local reactions) rather than judging by “feels different” the same day.
- Adjust only one variable at a time (dose before schedule, schedule before frequency changes).
Common limitations I’ve seen with GHK-Cu protocols
Because many “GHK-CU copper peptide dosage” discussions online are goal- and vendor-specific, users sometimes end up comparing protocols that aren’t actually comparable (different reconstitution volumes, different administration methods, different product purity/solvent details). That’s why I focus on dose math first—then protocol logic.
Product image reference (for identification)
FAQs
How do I use the ghk cu 50mg copper peptide dosage chart if my reconstitution volume isn’t listed?
Compute your concentration: 50mg ÷ total mL = mg/mL. Then multiply by your injected mL: (mg/mL) × (mL injected) = mg delivered. If you tell me your reconstitution volume and the syringe measurement you use (in mL), I can convert it into a clear per-dose mg number.
What injection volume should I choose for accurate dosing?
Choose a reconstitution volume that makes your target dose correspond to a syringe volume you can measure reliably. In my experience, reconstituting to around 5.0 mL (10 mg/mL) is often easier for incremental adjustments than very concentrated mixes like 1.0 mL, because small measurement errors translate into smaller mg swings.
Should I adjust dose based on skin changes day-to-day?
Skin responses can fluctuate due to hydration, irritation, and routine changes. I recommend evaluating progress over at least 1–2 weeks for clearer signal, while keeping dose and timing consistent during that interval. If you see persistent irritation at the injection site, treat that as a protocol warning sign and step back to a lower dose or pause while reviewing your process.
Conclusion: make your dosing math your “single source of truth”
The fastest way to stop guesswork with a GHK-Cu 50mg dosage chart is to anchor everything to concentration (mg/mL) and then calculate delivered mg from your injected volume. Once you do that, you can build a protocol with confidence: consistent timing, conservative ramping, and real logging—so your results are attributable to the dose, not measurement errors.
Next step: Choose your reconstitution volume, then use the matching table above (or the formula) to write down your exact mg per injection on a label or checklist before your first dose.
Discussion