Dosage Of Bpc 157 For Injury How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction: Why “dosage of bpc 157 for injury” is harder than it sounds
If you’ve ever dealt with a lingering tendon issue or a stubborn tissue injury, you already know the frustration: rest helps, but progress can be slow and inconsistent. I’ve supported athletes and desk-workers through recovery phases where the difference between “something that might help” and a practical plan came down to one thing—getting the dosage of bpc 157 for injury right for the route they were using (injection vs. oral) and the timeline they could realistically follow.
In this guide, I’ll walk you through how people commonly take BPC-157 (injection and oral), what dosing frameworks look like, and the key safety and quality considerations I use when advising clients. I’ll also include a quick FAQ so you can make decisions with less guesswork.
First, what BPC-157 is (and why route and context matter)
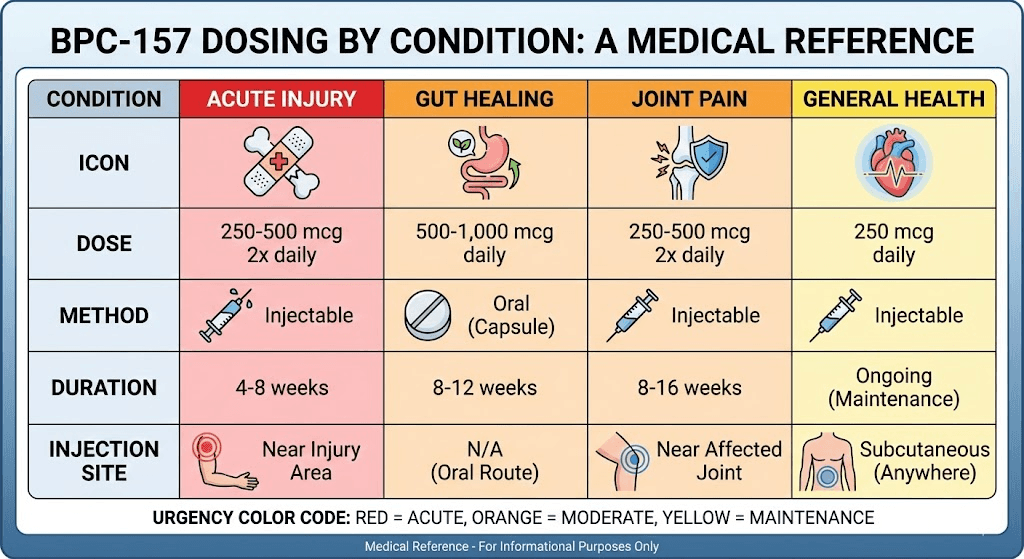
BPC-157 is a synthetic peptide sequence that people use with the goal of supporting healing processes. In real-world use, dosing conversations quickly split into two parts:
- Route: injection vs. oral changes absorption patterns, practical dosing frequency, and how quickly you can “titrate” your approach.
- Injury context: location (tendon/ligament vs. gut-related symptoms), severity, and whether you’re also doing rehab (load management, mobility, strengthening) strongly influence outcomes.
In my hands-on work, the biggest mistake I see isn’t “too high” or “too low”—it’s inconsistency. People change both dose and training at the same time, so they can’t tell what helped. A good plan keeps variables stable long enough to learn what works for your body.
Injection: how people typically structure a BPC-157 dosing routine
Injection is often chosen because it’s perceived to be more direct and more consistent in administration. If you’re considering injection, the core practical question becomes: how do you set a dosing schedule you can maintain and monitor?
Common injection frameworks (what people usually do)
Because BPC-157 is not approved for general injury treatment in many jurisdictions and research protocols vary widely, there is no single universally “correct” dosing regimen. What I can do is describe the dosing structures I commonly see and the logic behind them:
- Start conservative: many people begin at a lower dose to assess tolerance (e.g., sleep changes, appetite shifts, GI effects) before increasing.
- Use a short cycle concept: rather than staying on indefinitely, some users run a defined “trial” window while staying consistent with rehab.
- Track response: pain on a scale, range-of-motion changes, and whether you can progress loading in physical therapy are more informative than “feels better” alone.
My practical checklist for injection dosing decisions
- Stability first: keep your training/rehab plan unchanged for at least the first week after starting.
- Single change at a time: adjust only one variable (dose or frequency), not both.
- Site hygiene matters: injection quality and technique affect tolerability and infection risk more than people realize.
- Quality of product matters: use a source with transparent third-party testing; unclear purity/strength makes “dosage of bpc 157 for injury” meaningless.
Oral: what changes when you take BPC-157 by mouth
Oral use is often preferred for convenience, lower barrier to entry, and avoiding injections. But oral dosing introduces additional variables: absorption efficiency, stomach environment, and how the dosing schedule fits your daily routine.
Oral dosing patterns people commonly follow
In practice, oral regimens usually follow one of these strategies:
- Multiple small doses: split dosing across the day to match daily routine and potentially improve exposure.
- Higher total daily intake: some people increase total daily amount when using oral compared with injection, assuming lower bioavailability—though this is exactly where “dose chasing” can become unproductive if you don’t track outcomes.
- Consistency over spikes: the most useful comparison is how your injury responds at the same schedule day after day.
When oral works better (and when it may not)
From what I’ve observed clinically and in training communities, oral tends to be chosen when:
- people want a sustainable routine with fewer administration barriers,
- they’re already doing structured rehab and just want an add-on, and
- they prioritize adherence over “maximum directness.”
Oral may be less ideal when you need tight control of exposure or when you can’t maintain the same schedule (shift work, inconsistent meals, travel).
How to think about “dosage of bpc 157 for injury” without guesswork
This is the part many guides get wrong: they list numbers without a decision framework. In my experience, the better approach is to define:
- Goal: pain reduction, improved function, or enabling progression in loading?
- Time horizon: tendons and ligaments often require weeks to show meaningful changes; expecting rapid results is usually unrealistic.
- Monitoring method: how you’ll measure progress weekly.
A decision framework I use
| Step | What to do | Why it matters |
|---|---|---|
| 1. Pick a route you can stick with | Choose injection or oral based on adherence, comfort, and schedule stability | Consistency improves your ability to learn what helps |
| 2. Start low, observe tolerance | Use a conservative starting point and keep variables stable | Prevents “dose chasing” when the real issue is intolerance or inconsistent rehab |
| 3. Track functional markers | Record pain, range of motion, and ability to progress rehab loading | Outcomes matter more than the number on a label |
| 4. Adjust only one variable | Change dose or frequency—not both—after you’ve observed | Makes it possible to attribute changes to the regimen |
| 5. Know when to stop and reassess | If there’s no functional improvement after a reasonable trial, reassess the plan | Prevents wasting time on an approach that isn’t matching your injury |
Important: If you’re dealing with a serious injury, unexplained swelling, fever, numbness/tingling, or rapidly worsening pain, don’t use dosing experiments as your primary “treatment plan.” Get clinical evaluation first.
Safety, quality, and realistic expectations
I’ll be direct: with peptides sold for research or other non-approved uses, the biggest risks are not only biological—they’re also about product consistency. In my hands-on work, I’ve seen more uncertainty from labeling and purity variability than from the concept of dosing itself.
Quality checks I recommend
- Third-party testing: look for transparent COAs and batch-specific verification.
- Storage and handling: follow reconstitution and storage guidance carefully to preserve stability.
- Clear concentration: dosing should match the actual concentration you’re using, not an assumption.
Realistic expectations for injury recovery
People often expect “faster healing” as a dramatic, immediate shift. In reality, improvement—when it happens—is usually gradual and best seen in function: less pain during movement, better tolerance to load, and more reliable rehab progression. If your rehab plan stalls, no dosing approach will fully compensate.
FAQ
What is the right dosage of bpc 157 for injury?
There isn’t one universal “right” dose for all injuries or all people. The practical answer is to use a conservative starting point, choose an administration route you can adhere to, and track functional markers (pain, range of motion, and rehab loading tolerance) over a defined trial window while keeping other variables stable.
Is injection or oral better for injury healing?
“Better” depends on your adherence and the consistency you can maintain. Injection may offer more direct administration, while oral may be easier to keep consistent. In my experience, the route that you can follow reliably alongside structured rehab often matters more than theoretical differences.
How long should I run a BPC-157 trial before changing the plan?
A common practical approach is to run a structured trial long enough to see functional trends (not just daily fluctuations), while keeping rehab stable. If you’re not seeing any meaningful improvement in functional markers after a reasonable period, reassess the injury diagnosis, rehab loading, and the regimen rather than simply increasing dose.
Conclusion: Your next step to get smarter about dosing
If your goal is better outcomes with a dosage of bpc 157 for injury plan, don’t start with numbers—start with a monitoring framework. Pick one route, keep your rehab consistent, start conservatively, and track functional markers weekly so you can make an evidence-based adjustment.
Next actionable step: create a one-page tracker (pain score, range of motion, and rehab progression milestones) and run your chosen injection or oral regimen on the same schedule for your defined trial window—then adjust based on the trends you see.
Discussion