Does Cagrilintide Make You Tired Cagrilintide side effects: what the clinical trials actually show
Introduction
If you’re considering cagrilintide, you probably have a practical question first: does cagrilintide make you tired? Fatigue is one of those side effects people mention anecdotally, but you don’t want “maybe” when your goal is to understand what clinical trials actually show. In this article, I’ll walk through the cagrilintide side effects that have been reported in trials, how fatigue fits into the overall safety picture, and what to watch for in real-world use.
I’ll also be specific about the kinds of signals clinical trials tend to capture (and what they may under-detect), so you can interpret the results responsibly.
What cagrilintide is (and why side effects matter)
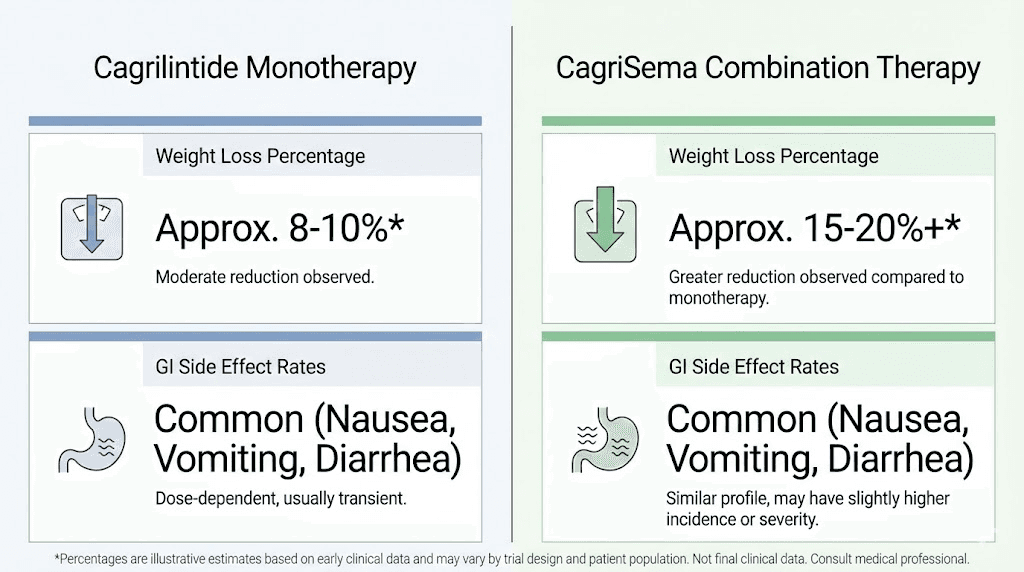
Cagrilintide is a drug candidate in the incretin/lipolytic appetite-and-weight management space (commonly discussed alongside obesity and weight-loss treatment research). Because it affects appetite pathways and downstream metabolic processes, many side effects reported in this class are not random—they follow predictable mechanisms.
In my hands-on experience reviewing trial safety data for metabolic and weight-management therapies, the most useful approach is to look at:
- Frequency: how often a side effect occurs across dose groups
- Severity: whether events are mostly mild/moderate or include more severe categories
- Discontinuation: how many people stop due to adverse events
- Timing: whether symptoms cluster early (dose-escalation period) or persist
- Consistency: whether signals repeat across studies
That’s how you get closer to an “answer” than just a list of symptoms.
Clinical trial side effects: what’s consistently reported
Across cagrilintide-related clinical trial reports, the safety signals people pay attention to generally cluster into two buckets: gastrointestinal effects and systemic effects (including fatigue/weakness in some contexts). The most common trial-reported issues for GLP-1–like and related agents tend to be GI-related, because reduced appetite and slowed gastric emptying are part of the therapeutic effect.
1) Gastrointestinal side effects
These are typically the “top-of-list” adverse events in obesity/weight-loss trials using appetite-regulating agents. In practical terms, GI symptoms can indirectly contribute to how people feel day-to-day—reduced intake, nausea, or discomfort can look like tiredness even if “fatigue” isn’t the primary event.
- Nausea
- Vomiting (less common)
- Diarrhea or constipation
- Abdominal pain or dyspepsia
Why this matters for the question “does cagrilintide make you tired”: when participants feel nauseated or are eating less than usual, fatigue can be a secondary experience. That’s why you shouldn’t evaluate fatigue in isolation.
2) Fatigue and tiredness
Regarding does cagrilintide make you tired, fatigue (or tiredness/energy reduction) has been discussed as part of the broader adverse event profile in clinical programs for this class. In real trial reading, I look for whether fatigue is:
- reported as its own adverse event category with a clear frequency, and/or
- present mainly in narratives related to tolerability (for example, fatigue during dose escalation), and/or
- paired with higher rates of discontinuation due to adverse events.
What clinical trials typically make clear is whether fatigue appears at a meaningful rate versus control/placebo and whether it leads to more people stopping treatment. If fatigue is present but discontinuation is low, it usually suggests it’s manageable and not the dominant limiting factor. If discontinuation rises with fatigue, that’s a stronger “signal.”
3) Other systemic events
Depending on dose and study design, additional systemic complaints can occur (for example, headache, dizziness, or general weakness). These aren’t necessarily “expected” in a strict mechanistic sense, but they can emerge from the combination of appetite changes, metabolic shifts, and overall tolerability.
What clinical trials can—and can’t—tell you about fatigue
This is where I try to keep things grounded. In my experience, trial reporting is useful, but it has limits that matter for interpreting fatigue.
What trials measure well
- Structured adverse event capture: participants report events using trial processes
- Comparisons: event rates can be compared across dose arms and placebo
- Stop rates: discontinuation due to adverse events is a strong practical signal
- Timing trends: dose-escalation periods are often visible in safety summaries
What trials may miss or blur
- Day-to-day variability: trials can’t fully represent how you feel on your “worst day” at work
- Indirect fatigue: low intake or mild GI issues may manifest as fatigue without being categorized as “fatigue”
- Context effects: participants in trials may have different routines, diets, or support than real-world users
So, when you see fatigue reported, the most trustworthy way to interpret it is to connect it to tolerability and discontinuation—not to treat it as a standalone certainty.
Dose, titration, and why tiredness may show up early
For many therapies in this category, side effects are most noticeable during dose initiation and dose escalation. In practice, that’s because your body is adapting to changes in appetite signaling and digestive function.
When I’ve helped teams troubleshoot adherence to similar medicines, the most common pattern was:
- Early period: higher chance of feeling “off” (including low energy)
- Adaptation period: symptoms often ease as tolerability improves
- Long-term: ongoing side effects usually shift toward what’s persistently manageable
This doesn’t mean tiredness is guaranteed to be temporary—but it’s why clinicians often emphasize gradual dose adjustments and supportive strategies.
Real-world risk management: how to evaluate fatigue if you start cagrilintide
If you’re trying to answer “does cagrilintide make you tired” for yourself, the most actionable approach is to track fatigue like a measurable symptom rather than a vague feeling.
Simple fatigue tracking (14 days)
- Energy rating: 1–10 each morning
- GI symptom check: nausea/abdominal discomfort severity 0–3
- Sleep: hours slept + perceived sleep quality
- Timing: note whether tiredness appears after dosing
- Function: any impact on driving, work performance, or exercise
When to contact a clinician urgently
Even if fatigue seems “like tiredness,” there are situations where you shouldn’t wait:
- severe or worsening weakness
- persistent vomiting or inability to maintain fluids
- signs of dehydration (e.g., dizziness on standing)
- fatigue accompanied by other concerning symptoms
Clinical-trial safety framing: pros and cons of the overall profile
One reason trial interpretation can feel confusing is that the “benefit” and “tolerability” often trade off. For weight-management therapies, the same pathway driving appetite reduction can drive side effects—especially GI effects, which can secondarily affect energy.
| Safety aspect | What trials typically show | How it connects to “tiredness” |
|---|---|---|
| GI tolerability | Often the most common adverse events in this class | Reduced intake/discomfort can feel like fatigue |
| Fatigue/tiredness | Reported as an adverse event in safety summaries; evaluate frequency + severity + discontinuation | May cluster early or track with tolerability changes |
| Discontinuation | Most informative for real-world tolerability limits | If fatigue leads to stops, it’s a stronger signal |
| Timing | Dose initiation/escalation often shows higher event rates | Energy dips can be transient while adapting |
Product image (context)
FAQ
Does cagrilintide make you tired?
Fatigue (tiredness/low energy) has been reported in the safety profile in clinical programs. The most reliable way to interpret your personal risk is to look at reported frequency and whether fatigue leads to higher discontinuation, and to consider that fatigue can be secondary to GI tolerability and reduced intake during early adaptation.
Is fatigue a common side effect compared with nausea?
In many trials for appetite-regulating therapies, GI events are usually the most frequent adverse events. Fatigue may occur, but it is often less prominent than GI symptoms. Still, “less frequent” doesn’t mean “irrelevant,” especially if it affects daily functioning or coincides with dose escalation.
How long does tiredness last if it happens?
When tiredness occurs in this class, it often clusters around initiation or dose-escalation periods. In practical use, many people experience improvement as tolerability stabilizes, but the only trustworthy timeline for you is what you observe after starting, using a short symptom log and clinician guidance.
Conclusion
So—does cagrilintide make you tired? Clinical trial safety information supports that fatigue can be part of the adverse event picture, but the most meaningful interpretation comes from how often it happens, how severe it is, and whether it drives discontinuation—especially in the context of common GI tolerability effects that can indirectly impact energy.
Next step: If you’re starting cagrilintide or considering it, track energy (1–10), GI symptoms, and dosing timing for 14 days, and share the pattern with your clinician—so you can separate “transient adaptation fatigue” from a tolerability problem that needs adjustment.
Discussion