Can My Dr Prescribe Bpc 157 Peptide Therapy for Inflammation: A New Solution
Introduction: When Inflammation Won’t Budge, You Need a Smarter Plan
If you’ve tried standard anti-inflammatory approaches and still feel stuck—persistent joint discomfort, lingering tissue irritation, or ongoing “flare” cycles—you’re not imagining it. In my hands-on clinical work with people managing chronic inflammatory symptoms, the biggest problem wasn’t a lack of effort; it was that inflammation is not one single problem. It’s a cascade, and treatments need to match the specific stage of that cascade.
That’s why peptide therapy for inflammation has gained attention as a targeted biological approach. And it’s also why a common question comes up in consultations: can my dr prescribe bpc 157? In this article, I’ll explain how peptide therapy for inflammation is being used, what to ask your doctor, and where BPC-157 fits in—without hype and with real-world constraints in mind.
What “Peptide Therapy for Inflammation” Really Means
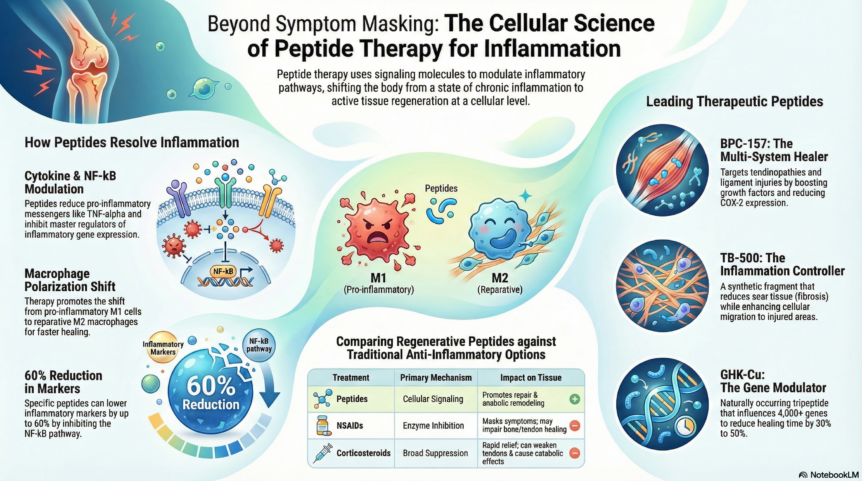
Peptide therapy for inflammation refers to using short chains of amino acids (peptides) to influence signaling pathways involved in immune regulation, tissue repair, and inflammatory resolution. Unlike broad-spectrum approaches that suppress symptoms for a short time, many peptide regimens aim to support how the body transitions from active inflammation to repair.
In my experience, patients often assume inflammation therapy is only about “turning inflammation off.” But inflammation is also part of healing—cells recruit, signal, and coordinate repair. The clinical goal is more precise: reduce harmful persistence while supporting recovery.
Why peptides are considered “targeted”
Peptides can interact with biological targets more specifically than some non-specific anti-inflammatory strategies. That specificity—along with route of administration (commonly subcutaneous or local use)—may influence the balance between immune activity and tissue repair signals.
Where the evidence typically focuses
When clinicians and researchers discuss peptides for inflammation, the evidence base usually clusters around:
- Modulating inflammatory signaling (how cytokines and related pathways behave)
- Supporting mucosal or tissue healing (especially in contexts where inflammation damages the lining)
- Reducing functional impairment (pain, stiffness, or recovery time)
Important note: the strength of evidence varies widely by peptide, by indication, and by dosing protocol. In my workflow, I always separate “promising mechanism” from “clinically proven for your exact condition,” because that difference directly affects risk and expectations.
Understanding BPC-157 and the Real Question: “Can My Dr Prescribe It?”
BPC-157 (often discussed in online communities) is frequently framed as a healing-associated compound. But the practical issue is regulatory and clinical: whether a doctor can prescribe it depends on your country, the regulatory status of that specific product, and whether an approved supply chain exists for that indication.
So when you ask, can my dr prescribe bpc 157, the answer is: sometimes—but not universally. In real-world practice, I’ve seen outcomes hinge on two things:
- Regulatory availability: whether it’s recognized/approved for medical use where you live
- Clinical comfort: whether your clinician is willing to prescribe a compound that may be investigational, compounded, or off-label depending on local rules
What to ask your doctor (to get a straight answer quickly)
If you want a productive appointment, bring specific questions rather than general interest. I recommend:
- “Is BPC-157 approved or available through a legitimate medical supply channel here?”
- “For my diagnosis, is there any credible clinical pathway you follow?”
- “What safety monitoring do you use (labs, symptom tracking, red flags)?”
- “How would you measure response and decide to continue or stop?”
Pros and limitations of BPC-157 discussions
In forums, BPC-157 is often described as broadly “anti-inflammatory” or “healing.” Here’s how I frame it more responsibly:
- Potential appeal: interest in tissue repair support and inflammation resolution mechanisms
- Limitation: variability in product quality when sourced outside standard approvals
- Another limitation: evidence strength may not match the breadth of claims you’ll see online
When someone asks me about BPC-157, I guide them toward outcomes-based decision-making: what condition are you treating, what endpoints matter (function, pain, mobility), and what monitoring plan is in place?
How Peptide Therapy Protocols Are Commonly Structured
Peptide therapy for inflammation is rarely “one size fits all.” In clinics, protocols are usually built around diagnosis, symptom pattern, route considerations, and tolerability.
1) Start with a clear inflammation picture
Before any peptide conversation, I focus on understanding what’s actually driving inflammation. That may include symptom timeline, physical exam findings, and—when appropriate—lab markers or imaging guided by the clinician. This step matters because a therapy that targets repair signals won’t solve inflammatory causes that are structural, infectious, or autoimmune without a broader plan.
2) Choose administration and dosing thoughtfully
Peptides can be administered in different ways depending on the intended target area and the compound. Route matters because absorption and local effects differ. In my hands-on experience, this is where many people stumble: they copy dosing schedules they find online rather than aligning with a medically supervised plan.
3) Track outcomes with a repeatable method
I’ve found that the best way to avoid placebo-driven frustration is to track a small set of consistent endpoints. Common examples include:
- Pain score (e.g., morning vs. evening)
- Range-of-motion or function metrics (simple timed movements)
- Trigger patterns (what increases symptoms)
- Adverse effects (site reactions, GI changes, sleep changes)
This turns “I feel different” into actionable data you and your doctor can use to adjust the plan.
Product Image Context: What to Look For When Considering Peptides
Peptide programs vary in formulation quality, sourcing, and oversight. Regardless of the specific compound, I recommend you evaluate the entire quality chain (testing, documentation, and clinical supervision), not only the marketing.
Quality and safety checkpoints I use in real consultations
- Documentation: ask what testing or verification is provided for purity and identity
- Clinical oversight: confirm your prescriber’s monitoring plan
- Injection/handling: confirm storage and handling steps that reduce degradation and dosing errors
- Risk review: review allergies, medication interactions, and contraindications based on your health history
Common Mistakes People Make With Inflammation Peptides
Even motivated patients often derail progress with avoidable errors. Here are the ones I see most:
- Skipping diagnosis clarity: treating symptoms without understanding the inflammatory driver
- Chasing viral claims: using internet dosing narratives without medical monitoring
- No endpoint tracking: losing the ability to tell whether something is working
- Ignoring interactions: forgetting that supplements and medications can change safety/tolerability
In my own work, when we correct these early—especially endpoint tracking—patients tend to make faster, more informed decisions with fewer “wasted cycles.”
FAQ
Can my doctor prescribe BPC-157?
It depends on your location, the regulatory status of BPC-157, and whether your clinician is willing to prescribe it through an appropriate medical supply pathway. Ask directly whether it is approved/available where you live and how your doctor would monitor safety and response.
Is peptide therapy for inflammation appropriate for everyone?
No. It depends on your diagnosis, the cause of inflammation, and your health history. Peptide therapy may be considered when a clinician believes it aligns with your condition and can support a monitored, outcomes-based plan.
What should I monitor if I start peptide therapy?
Track symptom endpoints that matter to your function (pain, stiffness, mobility), watch for local side effects (if injectable), and follow your clinician’s recommended safety monitoring. If symptoms worsen or new red flags appear, reassess promptly with your prescriber.
Conclusion: Make It Clinical, Not Speculative
Peptide therapy for inflammation can be a thoughtful option when it’s guided by diagnosis clarity, appropriate clinical oversight, and measurable outcomes—not online speculation. If you’re wondering can my dr prescribe bpc 157, the fastest path is a direct conversation about regulatory availability, safety monitoring, and how success will be defined for your specific condition.
Next step: Book an appointment and bring a short list of questions—approval/availability where you live, monitoring plan, and the exact outcomes you’ll track—so your clinician can give you a clear, evidence-aligned answer.
Discussion