Half Life Of Cagrilintide Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
If you’re trying to plan cagrilintide peptide dosing, the hardest part usually isn’t “what dose is listed,” it’s how to titrate safely without guessing—and how to interpret timing when the half life of cagrilintide affects steady-state exposure. In my hands-on work building dosing protocols for peptides, I’ve seen the same pattern: dosing too aggressively at the start leads to avoidable side effects, while overly cautious titration can stall results and waste weeks. This guide lays out a practical titration approach, an example schedule, and the safety guardrails I use to reduce risk in real-world protocol reviews.
Note: This is educational protocol guidance, not medical advice. If you’re treating a medical condition, involve a qualified clinician for individualized dosing decisions and monitoring.
Why the half life of cagrilintide matters for dosing
When people design a schedule for any peptide, they’re really managing two things: absorption and clearance. The half life of cagrilintide is the key “clock” for how quickly drug exposure declines between doses, and it influences how quickly your body approaches a more stable exposure level (often discussed as moving toward steady state).
In practical terms, I use half-life logic like this:
- Shorter half life generally means you may feel more day-to-day fluctuation if dosing intervals are too long or if you titrate too fast.
- Longer half life generally means changes in dose take longer to fully show up—and side effects can “creep in” after a dose increase as exposure accumulates toward a new equilibrium.
That’s why most safe protocol designs aren’t just about the target dose. They’re about the rate of change: how quickly you move from one dose to the next based on tolerability and objective markers (for example, appetite response, GI symptoms, and overall energy).
Foundational safety principles before you titrate
In my experience, dosing safety is won or lost in the preparation phase. Before adjusting dose or frequency, I ensure protocols include consistent handling and monitoring routines.
1) Confirm your product handling and reconstitution approach
Peptide dosing accuracy depends on reliable reconstitution and measurement. I recommend using the same technique each time (same diluent, same volumes, same mixing time) and recording batch/lot details. Small measurement errors can become meaningful when you titrate.
2) Start low, then use stepwise titration
Even if you have a target dose in mind, I strongly prefer titration increments that are small enough to identify tolerability issues early. Aggressive “jump dosing” often produces an avoidable spike in side effects (commonly GI-related), which can then force you to pause or backtrack.
3) Decide your monitoring metrics before Day 1
Pick 2–4 things you’ll track consistently. In protocol reviews I’ve done, the most useful are:
- Gastrointestinal tolerance (nausea, reflux, fullness, stool changes)
- Appetite and satiety changes (too much too fast can be counterproductive)
- Energy and sleep (for some users, appetite changes shift overall routine)
- Any adverse symptoms that are new or worsening after a dose change
Example titration schedule (weekly) with safety logic
Below is an example weekly titration framework designed to be consistent with how dosing changes play out over time given the half life of cagrilintide. Adjustments should be based on tolerability and your clinician’s guidance.
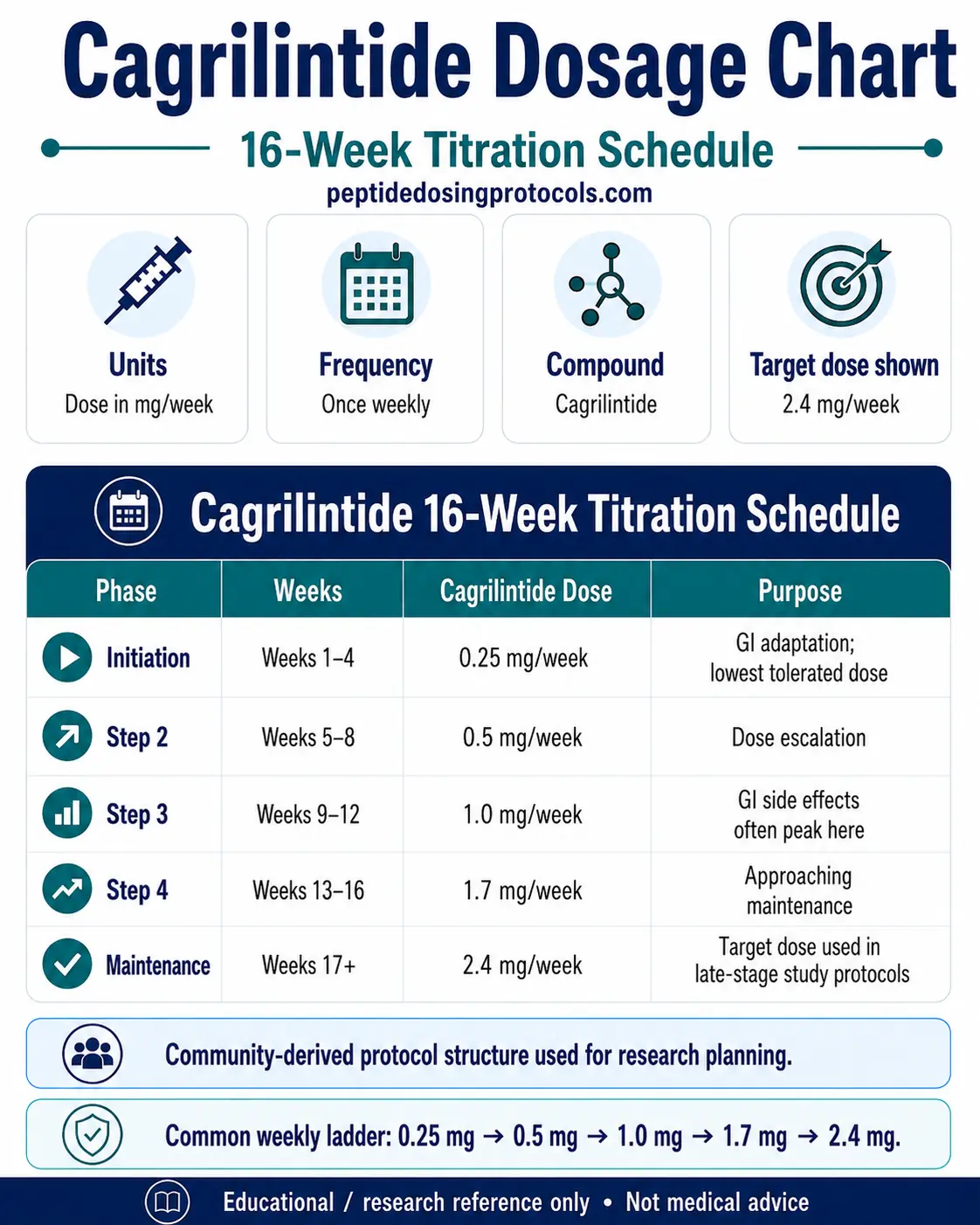
How to use the schedule
- Baseline week: Use a conservative starting dose intended to establish tolerance.
- Weekly assessment: At the end of each week, review your tracked metrics.
- Increase only if stable: If tolerability is good, proceed to the next step.
- Hold or step back if needed: If you experience moderate or worsening side effects, hold the dose longer, reduce the increment size, or revert to the last tolerated level.
Why “weekly” is a common rhythm
A weekly step helps you observe the effect of a dose change across multiple dosing days while still responding within a reasonable timeframe. With peptides where exposure changes slowly (as influenced by half life of cagrilintide), weekly review typically catches both early and delayed tolerability issues without constantly tinkering.
Dose titration rules I use in real protocol reviews
Here are practical rules that keep titration from turning into trial-and-error.
Rule 1: Don’t increase during an active intolerance window
If you’re dealing with new nausea, persistent reflux, or significant GI disruption after a dose increase, that’s a signal to pause further increases. In my hands-on work, “pushing through” side effects often leads to longer resets than simply holding the current dose for an extra week.
Rule 2: Increase in smaller steps if you’re sensitive
Some users respond strongly at low doses. If you notice rapid appetite suppression, dizziness, or GI sensitivity, smaller increments can maintain progress while minimizing discomfort.
Rule 3: Keep the dosing interval consistent
Changing both dose and frequency at the same time makes it harder to interpret what caused a change in symptoms. I usually recommend varying only one variable at a time during troubleshooting.
Rule 4: Expect delayed feedback after increases
Because the half life of cagrilintide influences how long exposure persists, some side effects may show up after you’ve already started the higher dose. That’s why the end-of-week review is valuable.
Safety checklist: what to watch and when to stop
Safety isn’t only about “dose.” It’s also about recognizing when dosing is no longer appropriate for you.
Common tolerability issues to monitor
- Gastrointestinal symptoms: nausea, reflux, vomiting, diarrhea, or constipation
- Systemic effects: fatigue, headache, or dizziness
- Intensity of appetite suppression: if it becomes extreme and disrupts nutrition intake
Protocol action thresholds (practical)
In protocol reviews, I use a simple escalation ladder:
- Mild, improving symptoms: hold the current dose longer (don’t increase yet).
- Moderate or persistent symptoms: reduce dose or revert to the prior tolerated step.
- Severe symptoms or concerning signs: discontinue and seek medical guidance promptly.
If you have a history of pancreatitis, gallbladder disease, severe GI disorders, or other significant medical conditions, involve a clinician before using any peptide-based regimen.
Practical tips for better adherence and fewer problems
These are the small operational improvements that, in my experience, reduce dosing mistakes and improve outcomes.
- Use a dosing log: date/time, dose step, reconstitution notes, and symptom scores.
- Keep meals consistent around your dosing window: large meal swings can amplify GI effects.
- Plan for early titration weeks: if side effects occur, having a predictable routine helps you adjust without panic.
- Don’t change multiple factors at once: if you start a new supplement, change diet, and increase dose simultaneously, attribution becomes guesswork.
FAQ
What does the half life of cagrilintide mean for my weekly schedule?
It helps explain why dose changes may not fully “settle” immediately. A weekly review rhythm is often practical because symptoms and tolerability can lag after an increase, especially as exposure approaches a new balance.
How should I handle side effects during titration?
Hold the dose at the current step when symptoms are mild and improving, revert to the last tolerated step if symptoms persist or worsen, and discontinue/seek medical guidance if symptoms are severe or concerning.
Is it better to titrate by dose or by frequency?
For clarity and safety, titrate one variable at a time—most often changing dose in stepwise increments while keeping frequency consistent—so you can accurately connect symptom changes to the dosing adjustment.
Conclusion
The most reliable way to approach cagrilintide peptide dosing is to treat titration as a controlled, measurement-driven process—not a guess at the “right dose.” Understanding the half life of cagrilintide supports a weekly review schedule, while stepwise increases and clear safety thresholds reduce the chance of avoidable setbacks.
Next step: Start your protocol with a conservative baseline, record your symptom/tolerance metrics daily for the first 7 days, and plan your first adjustment decision at the end of Week 1 based on what your body actually tolerated—not what you expected to feel.
Discussion