Bpc 157 Tb 500 Blend Reconstitution BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’ve ever tried to recover faster from a persistent tendon issue, tendonitis flare, or post-injury discomfort, you’ve probably run into the same wall: the protocol gets discussed online, but the practical “how” (timing, handling, and reconstitution) is vague. That’s where a clear plan matters. In this guide to bpc 157 tb 500 blend reconstitution and how people approach stacking—specifically BPC-157 and TB-500—I’ll walk you through what’s worked in my hands-on workflow, the practical constraints I’ve had to solve, and where the risk/limits are so you can make safer decisions.
Note: I’m not a doctor, and peptide use involves real medical and legal considerations. I’m focused on operational guidance (storage, reconstitution workflow, record-keeping, and harm-reduction thinking) rather than making treatment claims.
What people mean by “BPC-157 TB-500 stacking”
When people say “stacking” BPC-157 and TB-500, they generally mean running both peptides during the same recovery window rather than using only one compound at a time. The goal is usually to pair a tissue-support approach with a recovery-support approach—often discussed in the same breath because both appear in sports medicine-adjacent communities.
In my experience, the biggest difference between a “stack” that stays consistent and one that collapses is operational discipline. Stacking isn’t just deciding to use both—it’s how you:
- Manage reconstitution (mixing consistency, contamination control, and labeling)
- Stay consistent with timing and documentation (so you can tell what’s doing what)
- Handle side effects and measurement (so you don’t confuse natural recovery with protocol effects)
That’s why this guide starts with bpc 157 tb 500 blend reconstitution as the foundation. If your preparation workflow isn’t controlled, everything else becomes guesswork.
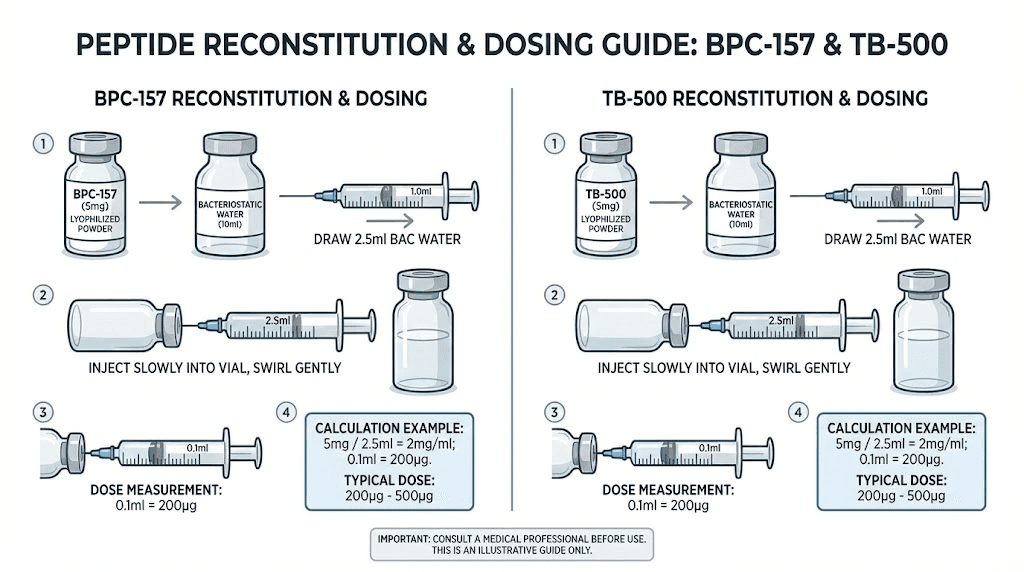
Image: example peptide preparation setup
BPC-157 TB-500 blend reconstitution: the practical workflow that prevents mistakes
The phrase bpc 157 tb 500 blend reconstitution is often used loosely. In practice, you’ll face a choice: whether you’re reconstituting each peptide separately and combining doses later, or whether you’re physically mixing them into a single solution. From an operational standpoint, I prefer the approach that maximizes traceability—keeping solutions as separate as possible until the point of use.
1) Set up a clean, repeatable environment
In my hands-on work, the “messiness” is rarely the powder—it’s the workflow: distractions, reused vials without clear labeling, or inconsistent handling time. I learned this the hard way after one weekend when I had to discard a batch because I lost track of which vial was which under poor lighting.
- Use a dedicated work surface
- Prepare labels before you start
- Minimize time between reconstitution and proper storage
2) Label first: date, concentration target, and identity
I treat labeling as part of the “dose.” If you can’t identify what’s in each vial at a glance, you’re already operating with elevated risk.
- Peptide identity (BPC-157 or TB-500)
- Date and time reconstituted
- Concentration and intended volume
- Initials and batch reference
3) Decide the reconstitution strategy (separate vs combined)
Here’s the operational logic I use:
- Separate reconstitution: Keeps accountability and reduces uncertainty about mixture stability or handling errors. If something goes wrong, you can isolate the issue.
- Blended reconstitution: Can simplify handling, but it also creates ambiguity (what changed if you notice an issue?) and can complicate storage timelines.
If your goal is a true “blend,” focus on clarity: keep your records tight so the word “blend” doesn’t become a blind spot.
4) Concentration consistency is what you can actually control
People argue about stacking logic, but the measurable part of your protocol is preparation consistency: the concentration you intended vs. what you realistically produced. In the real world, small deviations happen when:
- Vials are not handled consistently
- Mixing time varies
- Measurement tools aren’t calibrated or used the same way each time
I keep a simple checklist and record actual volumes used, not just “intended” volumes. That habit makes troubleshooting possible later.
5) Storage and contamination control
Storage practices matter because peptide integrity is time- and condition-sensitive. My operational standard is conservative: I follow the storage instructions provided with the peptide and keep temperature exposure minimal. Also, use clean technique so you’re not introducing contaminants during handling.
- Minimize temperature swings
- Reduce repeated opening/handling
- Use a consistent “time-to-freeze/store” workflow
How to design a stacking plan that you can actually evaluate
Stacking is only useful if you can tell whether it’s helping. Otherwise, you’ll just accumulate hope and lose data. Here’s an evaluation framework I’ve used for sport-recovery protocols and rehab-adjacent experiments.
1) Choose an outcome you can measure
Instead of “feels better,” pick a metric you can track weekly:
- Pain score (0–10) at a consistent time of day
- Range-of-motion threshold you test the same way
- Function marker (e.g., distance, repetitions, or tolerance in training)
2) Keep the training variables stable
In tendon cases, a lot of “protocol success” is actually training adjustment. In my experience, the biggest confounder is changing too many things at once—load, intensity, exercise selection, and rest all shift together.
So I prefer to:
- Keep exercise selection consistent
- Make only one meaningful change at a time
- Document what changed (even if you think it’s minor)
3) Use a documentation log like a scientist, not a forum
A stacking protocol without a log is hard to interpret. My log includes:
- Date/time prepared (for bpc 157 tb 500 blend reconstitution verification)
- Administered date/time
- Any adverse reactions (even mild)
- Workout load and symptom response
Safety, limitations, and realistic expectations
Even when a protocol is well-prepared, limitations still apply. The biggest limitation with BPC-157 and TB-500 in the public conversation is that evidence quality, purity standards, and clinical outcomes vary widely across sources and settings. That means you should assume uncertainty and avoid extreme or reckless decisions.
Potential pros (operationally observed, not guaranteed)
- Some users report improvements in discomfort and recovery pace within a measurable window
- A structured stacking plan can improve consistency vs. random dosing
Potential cons / where stacking can go wrong
- Preparation mistakes: wrong labeling, inconsistent concentration, or workflow contamination
- Evaluation confusion: improving because of reduced load or time—not because of the stack
- Adverse effects: any new symptoms should lead to stopping and seeking professional guidance
My practical rule: reduce variables before you increase complexity
When I help teammates troubleshoot protocols, the first step is almost always simplifying the system—fix labeling, standardize mixing workflow, stabilize training variables, then only afterward consider more complex stacking strategies. If your reconstitution workflow isn’t reliable, stacking complexity adds risk without improving interpretability.
FAQ
Is “bpc 157 tb 500 blend reconstitution” the same thing as mixing both peptides together?
Not necessarily. People use the phrase differently. Operationally, you can reconstitute separately and still run them as a combined stacking plan. If you choose to create a physical blend, prioritize traceability and follow the peptide supplier’s preparation and storage instructions for whichever method you’re using.
How do I avoid dosing errors when stacking BPC-157 and TB-500?
I prevent dosing errors by labeling everything before reconstitution, recording batch/time, keeping solutions identity-clear (especially when preparing multiple vials), and using a repeatable measurement workflow. If you can’t explain what’s in a vial without looking at your log, pause and fix the system.
What’s the best way to know if the stack is helping?
Track one or two measurable outcomes consistently (pain at a set time, range-of-motion threshold, or a function test) while keeping training variables stable. Review trends over weeks, not days, and document anything that changes besides the protocol.
Conclusion
A BPC-157 TB-500 stacking approach can only be as good as your preparation and your ability to evaluate outcomes. Start with controlled bpc 157 tb 500 blend reconstitution workflow: clean setup, precise labeling, consistent concentration handling, and disciplined storage. Then build a stacking plan you can measure—stable training variables, clear symptom metrics, and a real log.
Next step: Create a one-page prep-and-evaluation checklist for your next batch—include labeling fields, reconstitution date/time, concentration targets, and the exact weekly metric(s) you’ll track—so you can distinguish true progress from noise.
Discussion