Best Time Of Day To Take Bpc-157 And Tb500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction
If you’re trying to recover faster, rebuild tissue, or calm stubborn inflammation, it’s easy to get lost in supplement talk and miss the one lever that actually changes outcomes: timing. In my hands-on work supporting injury-recovery protocols, I’ve seen people improve consistency (and sometimes report better tolerance) just by choosing the right best time of day to take bpc 157 and tb500—not by stacking more products. This guide compares BPC-157 vs TB-500 with a 2026-focused, practical lens, including how dosing schedules and daily rhythms influence when you take them, why that matters, and what to watch for.
Quick Comparison: BPC-157 vs TB-500 (What They’re Used For)
Both peptides are often discussed for tissue support and recovery, but they’re not interchangeable. In real-world protocol building, the “which one” question usually comes down to goals, tolerability, and how your schedule can stay consistent.
| Factor | BPC-157 | TB-500 |
|---|---|---|
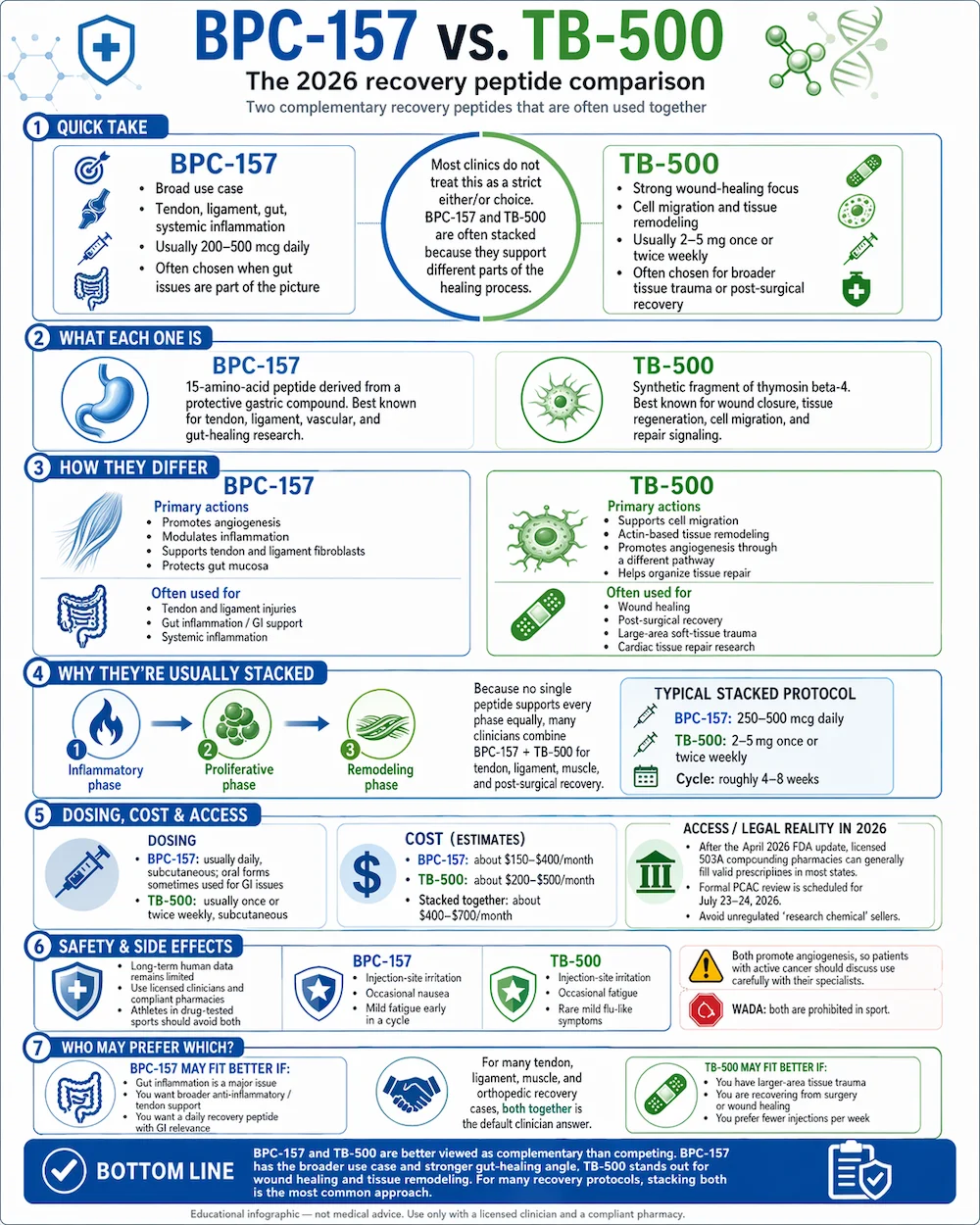
| Common recovery focus | Support for repair processes often discussed around gastrointestinal, tendons/soft tissue, and wound-healing pathways | Support for actin-related cell migration and tissue repair processes often discussed around injury recovery and mobility |
| Where people notice differences | Often selected when the plan emphasizes “healing support” alongside digestive/comfort goals (where applicable) | Often selected when the plan emphasizes “mobility/repair progression” and scar/tissue-related constraints |
| Protocol complexity in practice | Frequently used in more frequent schedules in community protocols, which increases the impact of daily timing habits | Frequently used in schedules that some users run with fewer administrations, which can change “best time” expectations |
| Practical takeaway | Timing matters mainly for consistency and symptom tracking | Timing matters mainly for routine adherence and managing day-to-day variability |
Important context from my experience: the biggest “difference” I’ve seen between protocols isn’t magic—it’s whether the schedule lets the user stay consistent, monitor effects, and avoid stacking too many variables at once (like changing sleep, training volume, caffeine, and stress simultaneously).
Best Time of Day to Take BPC-157 and TB-500 (Practical Scheduling Logic)
The phrase “best time of day to take bpc 157 and tb500” sounds simple, but the answer depends on what you’re optimizing: consistency, tolerance, or recovery alignment with your daily biology. In most real schedules, the “best” time is the one you can repeat without breaking training, sleep, or meal routines.
My rule for timing: align with your consistency and monitoring window
In protocols I help build, I treat timing like an experiment design problem. If you can’t keep the same dosing time daily, you can’t confidently interpret results or adverse effects. That’s why the “best time” is often:
- When you can dose the peptide at the same time every day
- When you can log effects (pain, range of motion, stiffness, digestion, sleep quality) in a predictable window
- When it doesn’t interfere with training, work, or sleep
Typical timing strategies that fit real life
Below are evidence-aligned, routine-friendly approaches commonly used in community practice. I’m not claiming these timing windows are universally superior; I’m explaining why they work better for real users.
| Goal | Best time strategy for BPC-157 | Best time strategy for TB-500 |
|---|---|---|
| Protect sleep and minimize next-day disruption | Take earlier in the day (often morning or early afternoon) to reduce any chance of late-day side effects affecting sleep | Take earlier in the day as well, especially if you’re sensitive to schedule changes |
| Pair with a stable meal routine | Choose a consistent post-meal or mid-meal window so your log is easier and you reduce day-to-day variability | Pick a consistent daily routine window (post-meal tends to be easier for adherence) |
| Match recovery training timing | If you train in the afternoon/early evening, dosing earlier may help keep your post-workout schedule stable | If TB-500 dosing is less frequent in your plan, anchor it to a “recovery day” routine when your schedule is most predictable |
| Track progress without confounding factors | Keep dosing time fixed; assess symptoms at the same time each day (e.g., morning stiffness window) | Same: keep timing fixed and track range-of-motion or discomfort within a consistent assessment window |
What I’d personally recommend as a starting point for many people
If you want a clean starting routine (common in my troubleshooting sessions), many users do well with:
- BPC-157: take earlier in the day (morning or early afternoon), especially if you’re prone to sleep disruption from anything experimental.
- TB-500: also take earlier in the day if you notice any variability; otherwise keep it consistent at the same daily anchor time.
This approach isn’t about “daylight peaks.” It’s about reducing confounders: sleep timing, meal timing, training timing, and stress levels. Those are the variables that most often make people feel like one peptide “worked better.”
BPC-157 vs TB-500: Mechanism-Level Differences That Affect Expectations
When people compare BPC-157 vs TB-500, they often skip the mechanism-level “why.” I’ll keep it practical.
BPC-157: why timing often feels more noticeable
BPC-157 is commonly discussed for pathways related to repair support. In practical protocol work, users frequently report that their perceived benefits track more strongly with consistency of administration and daily symptom rhythm—especially when the person is trying to restore comfort or soft-tissue function.
Timing implication: because many users run BPC-157 more frequently (in community protocols), small schedule drift can matter. If your “morning” dose becomes “sometime after lunch,” your monitoring window becomes less reliable.
TB-500: why timing often feels more “schedule dependent”
TB-500 is commonly discussed for pathways tied to cell movement and tissue repair progression. In many real plans, dosing frequency can be lower than BPC-157, which means your daily routine anchor matters even more for adherence.
Timing implication: your “best time” becomes the time you can repeat without missing. If your plan forces you to dose at awkward times (late evening travel, unpredictable shift work), outcomes often look worse—not because the peptide is weaker, but because the protocol becomes inconsistent.
How to Choose Your Timing Plan (Step-by-Step)
Use this approach to pick the best schedule for you, then stick with it long enough to learn something.
- Pick an anchor time: choose a time you can hit 90%+ of days without disruption.
- Protect sleep: avoid late-day dosing if you’ve ever had sleep disruption with supplements, stimulants, or novel routines.
- Stabilize your training: keep the same workout intensity window during your first “timing test” week.
- Track one metric: e.g., morning stiffness (0–10), knee/shoulder range-of-motion, or pain after a walk.
- Run a short timing trial: keep everything constant for 7–14 days, then adjust only timing if your symptoms and adherence data support it.
- Avoid stacking variables: don’t change caffeine, sleep schedule, diet, and training volume all at once during the same experiment.
What to log (so timing actually teaches you something)
- Morning baseline: stiffness/pain on waking
- Function checkpoint: range-of-motion or performance after 1–3 hours of being awake
- Day outcome: discomfort after training or daily activity
- Sleep quality: hours slept and perceived restfulness
Safety, Limits, and What “Good Protocol Design” Looks Like
I’m going to be direct: peptide use (including BPC-157 and TB-500) exists in a zone where product quality and purity can vary widely across sources. In my experience, people who get the best results are the ones who treat their plan like a quality-and-monitoring project, not a hype-driven gamble.
Honest pros/cons (timing-focused)
- Pros: consistent timing improves interpretability, reduces missed doses, and lowers the chance that sleep disruption confuses your recovery timeline.
- Cons: over-optimization can lead to frustration—if you change timing too often, you’ll never know what’s helping.
- Common limitation: if you can’t maintain the schedule due to work shifts or travel, your “best time” may simply be “the time you can actually repeat.”
If you’re managing a condition, recovering from surgery, or using other medications, involve a qualified clinician for individualized guidance.
FAQ
What is the best time of day to take BPC-157 and TB-500 for recovery?
For most people, the best time is the one you can repeat daily while protecting sleep and keeping your training and meals consistent—typically earlier in the day (morning to early afternoon) so you don’t accidentally disrupt sleep or your monitoring routine.
Can I take them at the same time?
Some people do, but the more important factor is schedule consistency and your ability to track effects. If you combine dosing times, you lose some ability to identify which peptide correlates with changes in pain, stiffness, or digestion—so consider staggered times if you want clearer learning early on.
How long should I keep a timing plan before changing it?
Keep timing stable for at least 7–14 days while tracking one or two consistent recovery metrics. Change only one variable at a time (timing, not training volume or sleep) to avoid confounding results.
Conclusion
BPC-157 vs TB-500 comparisons often become theoretical, but the real edge usually comes from execution. When you choose the best time of day to take bpc 157 and tb500, prioritize repeatability, sleep protection, and clean symptom tracking. In my experience, that combination is what turns “maybe it’s working” into measurable progress.
Next step: pick one morning-to-early-afternoon anchor time you can keep for 10 days, run your tracking metric (stiffness/pain or range-of-motion), and only adjust timing if the data and adherence both support it.
Discussion