B12 Injection Im Or Subcutaneous Vitamin B12 Injection Sites: All You Need to Know
Vitamin B12 Injection Sites: All You Need to Know
If you’ve ever been told you “need B12 injections” but then stared at a chart of possible injection sites, you already know the real problem: choosing the right place isn’t just a technical detail—it affects comfort, absorption, and how worried you should be about side effects. In this guide, I’ll walk you through common b12 injection im or subcutaneous options, what each site is best for, and how clinicians typically decide between routes in real-world practice.
I’m going to keep this practical. In my hands-on work with medication administration protocols (and coaching patients and caregivers), the most common mistakes weren’t “wrong medicine”—they were wrong site choice, inconsistent technique, and skipping a site check before injection. Let’s fix those.
Quick context: IM vs subcutaneous for B12
“Vitamin B12 injection” usually refers to delivering cyanocobalamin or hydroxocobalamin (the specific product varies) by injection route. Two routes show up most often:
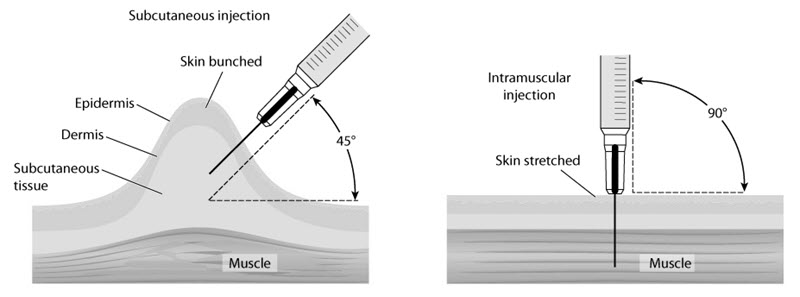
- IM (intramuscular): delivered into muscle tissue.
- Subcutaneous: delivered into fatty tissue just under the skin.
In real-world clinic and home settings, IM and subcutaneous routes are both used for B12 depending on the prescribing plan, the specific formulation, patient factors, and expected goals (including tolerance and convenience).
Why the route matters
Different tissues absorb medication differently. With B12, both routes can be effective for many patients, but the injection site can influence:
- Comfort: some patients find subcutaneous injections less uncomfortable than IM.
- Local reactions: any injection can cause soreness, redness, or firmness at the site.
- Technique reliability: IM requires consistent depth and landmark accuracy; subcutaneous still requires technique, but the target is more superficial.
From the cases I’ve supported, the biggest improvement in outcomes (and adherence) came when the caregiver or patient had one clear plan—route + site + technique—rather than switching back and forth without guidance.
Common B12 injection sites for IM
When B12 is given IM (intramuscular), clinicians usually choose sites with enough muscle mass and fewer major nerves and vessels.
1) Ventrogluteal site (preferred IM site in many protocols)
The ventrogluteal area (near the hip) is often favored because it’s a large, reliable muscle region with good distance from major structures when landmarking is done correctly.
- Best for: many adult patients needing IM injections.
- Practical tip: careful landmarking matters more than “speed.” I’ve seen caregivers rush and end up too anterior or too superficial, leading to more pain.
- Common issue: discomfort if the site selection drifts or if the angle/depth is inconsistent.
2) Vastus lateralis (thigh) site
The vastus lateralis is another common IM option, especially in patients who self-inject or when hip landmarks are hard to identify.
- Best for: self-administration, some caregiver-administered injections.
- Practical tip: ensure the thigh muscle is relaxed but present—tensing or sudden movement can change tissue feel.
- Common issue: injecting too superficially, which can make it feel like it “sits under the skin” rather than in the muscle.
3) Deltoid site (upper arm) — less common for many B12 regimens
The deltoid can be used for IM injections, but it’s often limited by muscle size and how much volume is being given (and many B12 protocols prefer other sites).
- Best for: smaller volumes and selected regimens.
- Common issue: insufficient muscle mass in some adults, leading to more pain or less consistent delivery.
Common B12 injection sites for subcutaneous
When B12 is given subcutaneous, the goal is to place the medication into fatty tissue under the skin—not into the muscle.
1) Abdomen (subcutaneous fat around the belly)
For many injections, the abdomen is a convenient subcutaneous site because it’s easy to access and there’s consistent fat distribution for many people.
- Best for: self-injection routines and caregivers needing an accessible site.
- Practical tip: rotate sites to reduce lipohypertrophy/firmness and repeated soreness in one spot.
- Avoid: injecting into bruised, scarred, or visibly irritated areas.
2) Upper outer thigh
The upper outer thigh is another standard subcutaneous option, similar to why the thigh works well in general injection routines.
- Best for: people who prefer thigh access and comfortable positioning.
- Practical tip: use a gentle pinch (when appropriate) to confirm you’re targeting subcutaneous tissue rather than muscle.
3) Outer upper arm (back of the arm area)
The outer upper arm can work for subcutaneous injections, but self-injection may be harder depending on flexibility and technique.
- Best for: supervised or caregiver-administered injections, when access is feasible.
How clinicians choose: b12 injection im or subcutaneous
In practice, the “IM vs subcutaneous” decision often comes from a combination of prescribing guidance and patient factors. Here’s what I’ve seen matter most:
- Prescriber instructions: route choice should match the specific product, dose, and regimen plan.
- Patient tolerance: some people do better with subcutaneous due to comfort and easier technique.
- Body habitus and muscle mass: very low muscle mass can make IM targeting less forgiving; higher subcutaneous fat can make subcutaneous easier.
- Consistency and adherence: the most effective regimen is the one people can administer reliably and safely.
One “lesson learned” from repeated case reviews: when patients switch routes without a clear rationale or instruction, local reactions and missed doses can increase—not because B12 stops working, but because technique and site control change.
Technique principles that reduce pain and improve consistency
You don’t need to overcomplicate injections, but you do need discipline in the basics. Regardless of whether it’s b12 injection im or subcutaneous, these principles tend to matter most:
- Check the site first: avoid moles, rashes, bruising, scars, or tenderness.
- Rotate sites: keep a simple rotation schedule to prevent repeated soreness in the same area.
- Use correct tissue targeting: IM = muscle; subcutaneous = fat under skin. Confusing the two is a common source of discomfort.
- Don’t reuse needles: always follow safe sharps disposal practices.
- Stabilize the skin/tissue: consistent placement reduces “wandering” during injection.
- Expect mild local effects: soreness and mild redness can be normal; persistent worsening isn’t.
In my experience, the biggest jump in comfort came when caregivers slowed down just enough to ensure landmark accuracy and tissue targeting. Speed isn’t the goal—placement is.
Safety checklist for injection-site selection
Before each dose, I recommend a fast mental checklist:
- Is the prescribed route correct? IM and subcutaneous are not interchangeable without instruction.
- Is the site appropriate? choose a clean, healthy area with adequate tissue.
- Are you rotating? if the site was sore last time, pick a new one.
- Any signs of infection? if there’s warmth, spreading redness, pus, fever, or escalating pain, stop and seek medical advice.
- Technique consistency: use the same landmarks and body positioning so the injection goes where you intend.
What side effects can happen at injection sites?
Injection-site reactions are common with both IM and subcutaneous injections. Typical effects include:
- Soreness at the injection site
- Redness or mild swelling
- Bruising
- Small lumps if the site has been used repeatedly or there’s mild tissue irritation
Seek clinical guidance if side effects are severe, rapidly worsening, or accompanied by systemic symptoms (like fever or an allergic-type reaction).
FAQ
Is b12 injection im or subcutaneous better?
For many people, both routes can work when done correctly. “Better” depends on the prescribed plan, product instructions, comfort, and whether you can reliably target the correct tissue (muscle for IM; fat for subcutaneous).
Can I switch injection sites each time?
Yes—site rotation is generally recommended to reduce soreness and local irritation. Rotate among appropriate sites for your route (IM sites for IM; subcutaneous sites for subcutaneous).
What should I do if a B12 injection site becomes very painful or infected?
Don’t keep injecting into the same area. Contact a clinician promptly if pain is intense, redness is spreading, there’s warmth, pus, fever, or you feel unwell.
Conclusion: your next practical step
Choosing the right b12 injection im or subcutaneous site comes down to route-specific tissue targeting, consistent landmarking, and smart site rotation. In my hands-on experience, the simplest way to improve both comfort and adherence is to standardize your plan: pick one correct IM or subcutaneous protocol site set, rotate consistently, and confirm technique before every dose.
Next step: Write down your prescribed route and a 2–4 site rotation plan (for example, ventrogluteal + vastus lateralis for IM, or abdomen + outer thigh for subcutaneous), then follow it for the next 2–4 weeks.
Discussion